

Population-based study of disability and institutionalization after transient ischemic attack and stroke: 10-year results of the Oxford Vascular Study
- PMID: 23920019
- PMCID: PMC4946627
- DOI: 10.1161/STROKEAHA.113.001584
Population-based study of disability and institutionalization after transient ischemic attack and stroke: 10-year results of the Oxford Vascular Study
Abstract
Background and purpose: Long-term outcome information after transient ischemic attack (TIA) and stroke is required to help plan and allocate care services. We evaluated the impact of TIA and stroke on disability and institutionalization over 5 years using data from a population-based study.
Methods: Patients from a UK population-based cohort study (Oxford Vascular Study) were recruited from 2002 to 2007 and followed up to 2012. Patients were followed up at 1, 6, 12, 24, and 60 months postevent and assessed using the modified Rankin scale. A multivariate regression analysis was performed to assess the predictors of disability postevent.
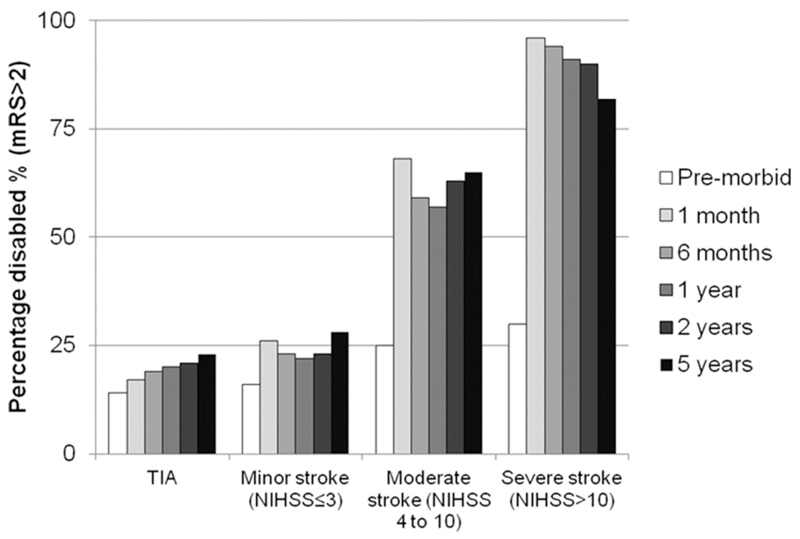
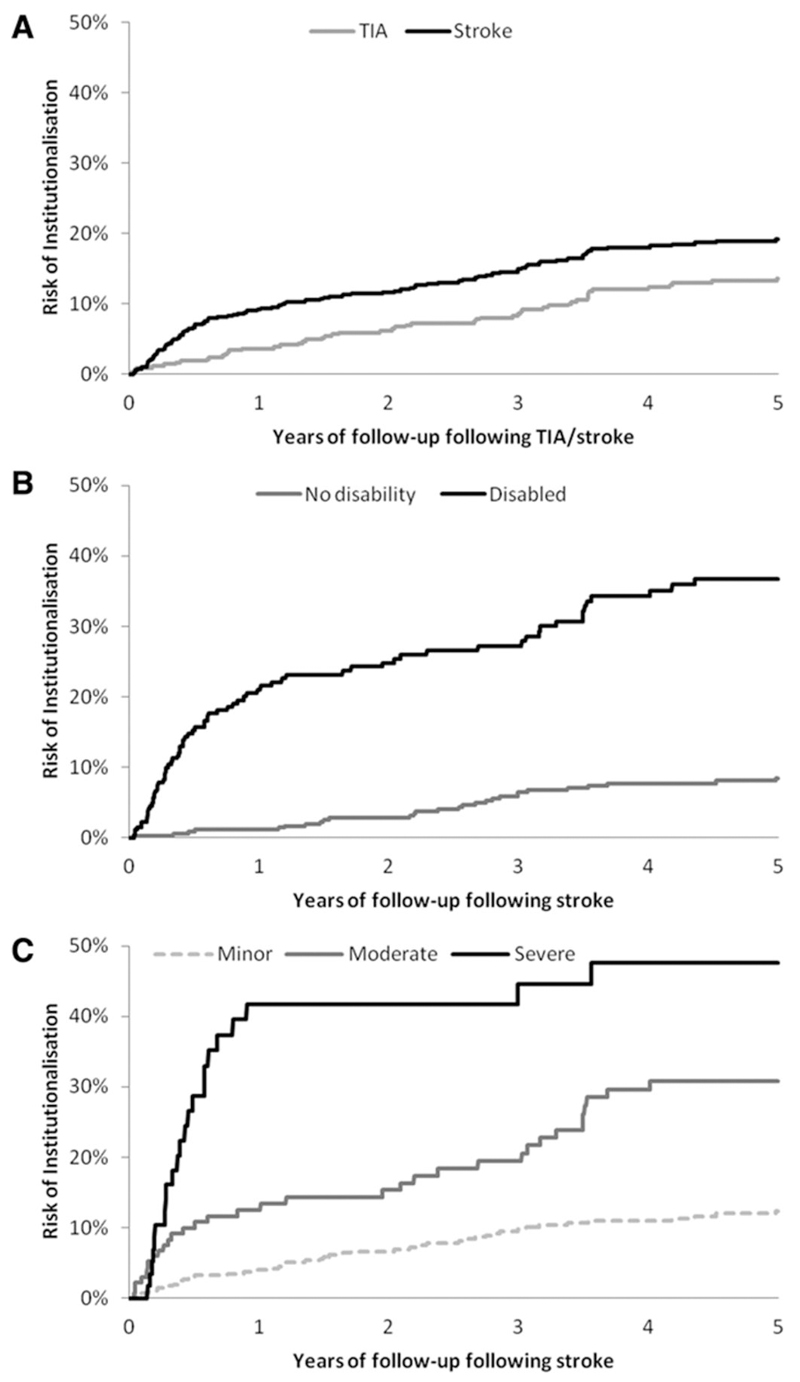
Results: A total of 748 index stroke and 440 TIA cases were studied. For patients with TIA, disability levels increased from 14% (63 of 440) premorbidly to 23% (60 of 256) at 5 years (P=0.002), with occurrence of subsequent stroke being a major predictor of disability. For stroke survivors, the proportion disabled (modified Rankin scale >2) increased from 21% (154 of 748) premorbidly to 43% (273 of 634) at 1 month (P<0.001), with 39% (132 of 339) of survivors disabled 5 years after stroke. Five years postevent, 70% (483 of 690) of patients with stroke and 48% (179 of 375) of patients with TIA were either dead or disabled. The 5-year risk of care home institutionalization was 11% after TIA and 19% after stroke. The average 5-year cost per institutionalized patient was $99,831 (SD, 67 020) for TIA and $125,359 (SD, 91 121) for stroke.
Conclusions: Our results show that 70% of patients with stroke are either dead or disabled 5 years after the event. Thus, there remains considerable scope for improvements in acute treatment and secondary prevention to reduce postevent disability and institutionalization.
Keywords: ischemic attack, transient; long-term outcome; nursing homes; stroke.
Conflict of interest statement
Disclosures: None.
Figures
References
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–1757. - PubMed
-
- Epidemiology of Stroke. Cerebrovasc Dis. 1999;9:1–68.
-
- Rothwell PM, Coull AJ, Giles MF, Howard SC, Silver LE, Bull LM, et al. Change in stroke incidence, mortality, case-fatality, severity, and risk factors in Oxfordshire, UK, from 1981 to 2004 (Oxford Vascular Study) Lancet. 2004;363:1925–1933. - PubMed
-
- Feigin VL, Van der Hoorn S. How to study stroke incidence. Lancet. 2004;363:1920. - PubMed
-
- Feigin VL, Lawes CMM, Bennett DA, Barker-Collo SL, Parag V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol. 2009;8:355–369. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
