Aetiological overlap between obsessive-compulsive and depressive symptoms: a longitudinal twin study in adolescents and adults
- PMID: 23920118
- PMCID: PMC3959155
- DOI: 10.1017/S0033291713001591
Aetiological overlap between obsessive-compulsive and depressive symptoms: a longitudinal twin study in adolescents and adults
Abstract
Background: Depression is commonly co-morbid with obsessive-compulsive disorder (OCD). However, it is unknown whether depression is a functional consequence of OCD or whether these disorders share a common genetic aetiology. This longitudinal twin study compared these two hypotheses.
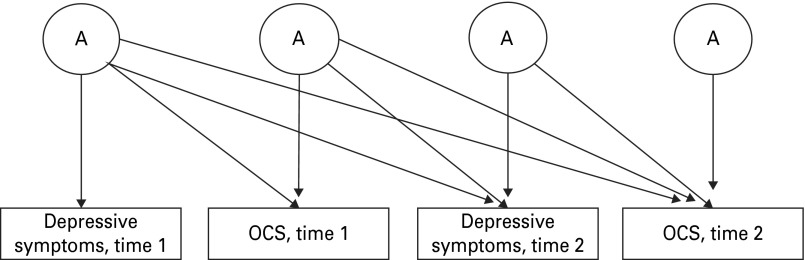
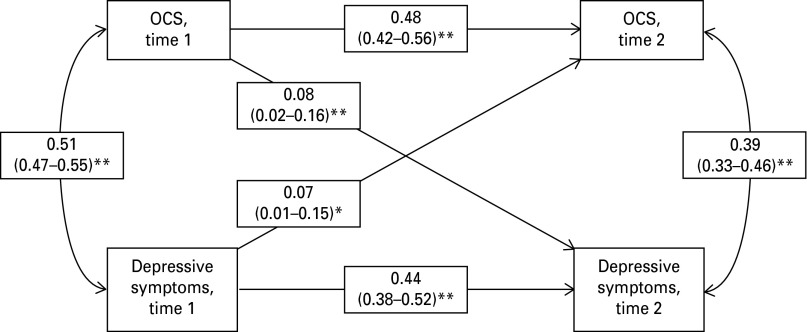
Method: Data were drawn from a longitudinal sample of adolescent twins and siblings (n = 2651; Genesis 12-19 study) and from a cross-sectional sample of adult twins (n = 4920). The longitudinal phenotypic associations between OCD symptoms (OCS) and depressive symptoms were examined using a cross-lag model. Multivariate twin analyses were performed to explore the genetic and environmental contributions to the cross-sectional and longitudinal relationship between OCS and depressive symptoms.
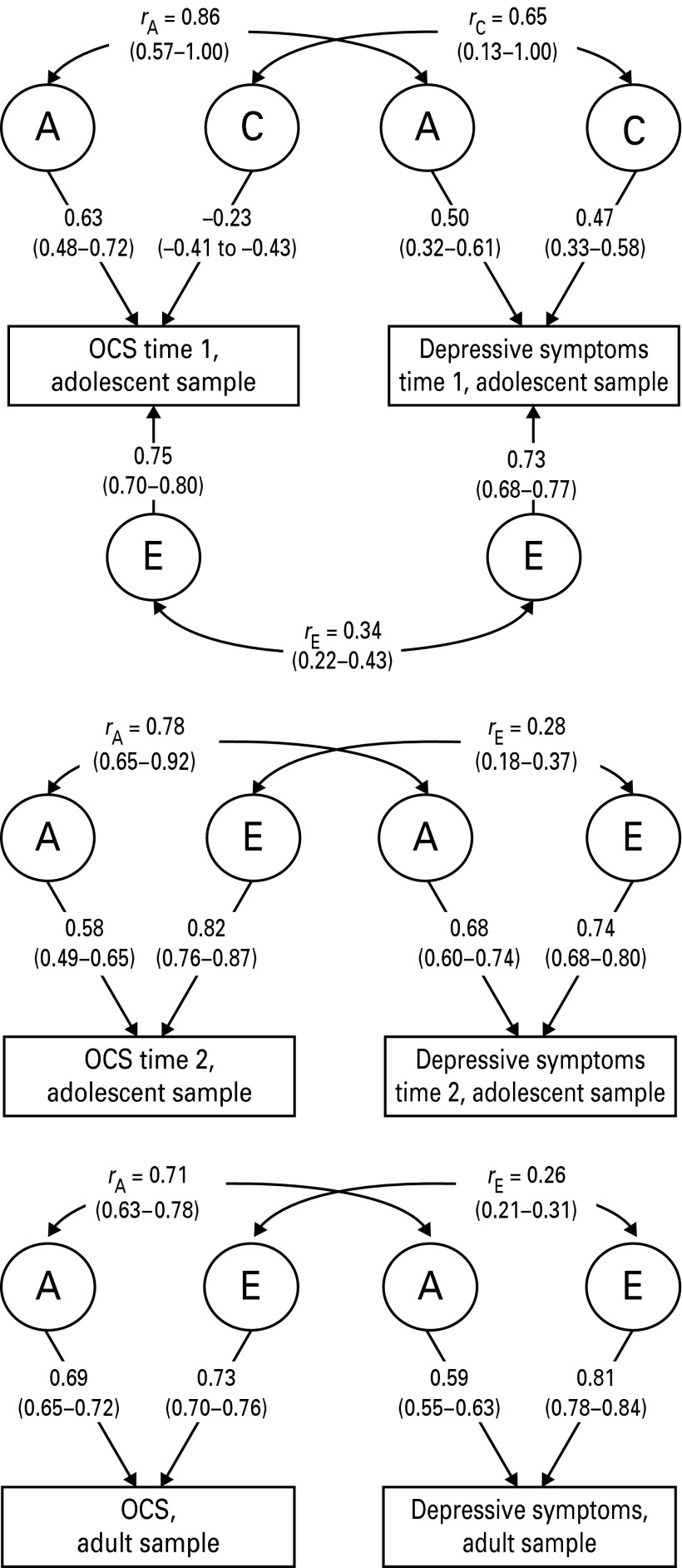
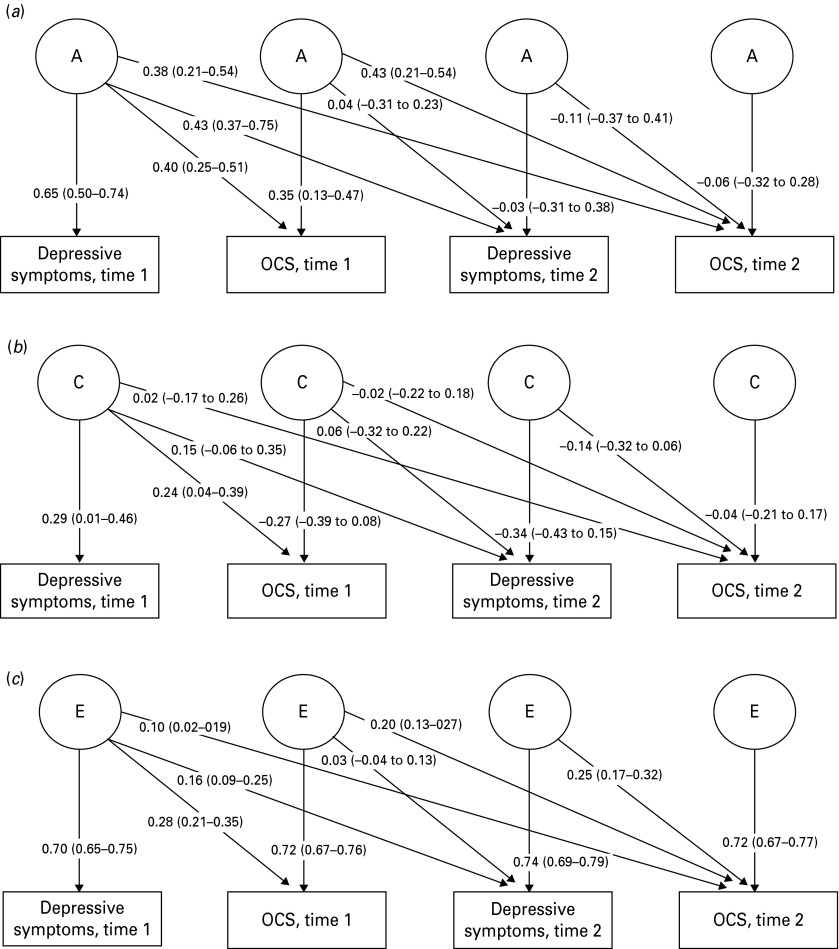
Results: In the longitudinal phenotypic analyses, OCS at time 1 (wave 2 of the Genesis 12-19 study) predicted depressive symptoms at time 2 (wave 3 of the Genesis 12-19 study) to a similar extent to which depressive symptoms at time 1 predicted OCS at time 2. Cross-sectional twin analyses in both samples indicated that common genetic factors explained 52-65% of the phenotypic correlation between OCS and depressive symptoms. The proportion of the phenotypic correlation due to common non-shared environmental factors was considerably smaller (35%). In the adolescent sample, the longitudinal association between OCS at time 1 and subsequent depressive symptoms was accounted for by the genetic association between OCS and depressive symptoms at time 1. There was no significant environmental association between OCS and later depressive symptoms.
Conclusions: The present findings show that OCS and depressive symptoms co-occur primarily due to shared genetic factors and suggest that genetic, rather than environmental, effects account for the longitudinal relationship between OCS and depressive symptoms.
Figures
References
-
- Abramowitz JS, Deacon BJ (2006). Psychometric properties and construct validity of the Obsessive–Compulsive Inventory–Revised: replication and extension with a clinical sample. Journal of Anxiety Disorders 20, 1016–1035 - PubMed
-
- Angold A, Costello EJ, Messer SC, Pickles A, Winder F, Silver D (1995). The development of the short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research 5, 237–249
-
- Anholt GE, Aderka IM, van Balkom AJ, Smit JH, Hermesh H, de Haan E, van Oppen P (2011). The impact of depression on the treatment of obsessive–compulsive disorder: results from a 5-year follow-up. Journal of Affective Disorders 135, 201–207 - PubMed
-
- Besiroglu L, Uguz F, Saglam M, Agargun MY, Cilli AS (2007). Factors associated with major depressive disorder occurring after the onset of obsessive–compulsive disorder. Journal of Affective Disorders 102, 73–79 - PubMed
-
- Bienvenu OJ, Samuels JF, Wuyek LA, Liang KY, Wang Y, Grados MA, Cullen BA, Riddle MA, Greenberg BD, Rasmussen SA, Fyer AJ, Pinto A, Rauch SL, Pauls DL, McCracken JT, Piacentini J, Murphy DL, Knowles JA, Nestadt G (2012). Is obsessive–compulsive disorder an anxiety disorder, and what, if any, are spectrum conditions? A family study perspective. Psychological Medicine 42, 1–13 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical