

Stroke in heart failure in sinus rhythm: the Warfarin versus Aspirin in Reduced Cardiac Ejection Fraction trial
- PMID: 23921215
- PMCID: PMC4256381
- DOI: 10.1159/000352058
Stroke in heart failure in sinus rhythm: the Warfarin versus Aspirin in Reduced Cardiac Ejection Fraction trial
Abstract
Background: The Warfarin versus Aspirin in Reduced Cardiac Ejection Fraction trial found no difference between warfarin and aspirin in patients with low ejection fraction in sinus rhythm for the primary outcome: first to occur of 84 incident ischemic strokes (IIS), 7 intracerebral hemorrhages or 531 deaths. Prespecified secondary analysis showed a 48% hazard ratio reduction (p = 0.005) for warfarin in IIS. Cardioembolism is likely the main pathogenesis of stroke in heart failure. We examined the IIS benefit for warfarin in more detail in post hoc secondary analyses.
Methods: We subtyped IIS into definite, possible and noncardioembolic using the Stroke Prevention in Atrial Fibrillation method. Statistical tests, stratified by prior ischemic stroke or transient ischemic attack, were the conditional binomial for independent Poisson variables for rates, the Cochran-Mantel-Haenszel test for stroke subtype and the van Elteren test for modified Rankin Score (mRS) and National Institute of Health Stroke Scale (NIHSS) distributions, and an exact test for proportions.
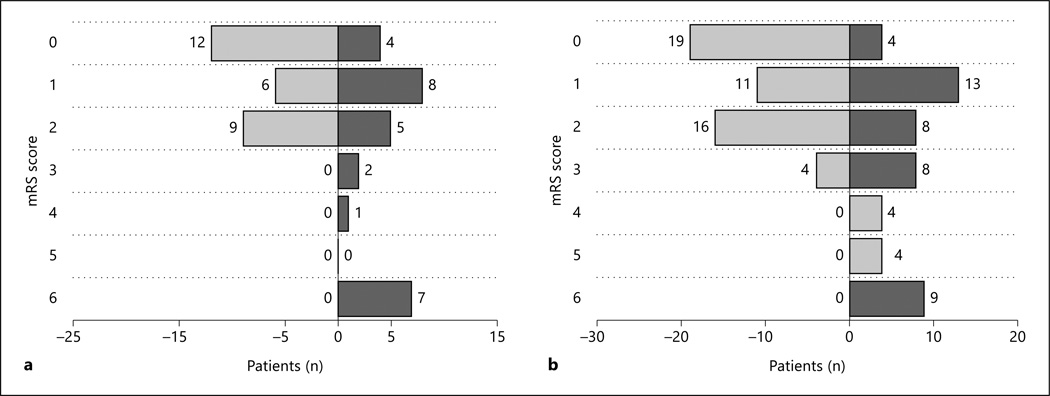
Results: Twenty-nine of 1,142 warfarin and 55 of 1,163 aspirin patients had IIS. The warfarin IIS rate (0.727/100 patient-years, PY) was lower than for aspirin (1.36/100 PY, p = 0.003). Definite cardioembolic IIS was less frequent on warfarin than aspirin (0.22 vs. 0.55/100 PY, p = 0.012). Possible cardioembolic IIS tended to be less frequent on warfarin than aspirin (0.37 vs. 0.67/100 PY, p = 0.063) but noncardioembolic IIS showed no difference: 5 (0.12/100 PY) versus 6 (0.15/100 PY, p = 0.768). Among patients experiencing IIS, there were no differences by treatment arm in fatal IIS, baseline mRS, mRS 90 days after IIS, and change from baseline to post-IIS mRS. The warfarin arm showed a trend to a lower proportion of severe nonfatal IIS [mRS 3-5; 3/23 (13.0%) vs. 16/48 (33.3%), p = 0.086]. There was no difference in NIHSS at the time of stroke (p = 0.825) or in post-IIS mRS (p = 0.948) between cardioembolic, possible cardioembolic and noncardioembolic stroke including both warfarin and aspirin groups.
Conclusions: The observed benefits in the reduction of IIS for warfarin compared to aspirin are most significant for cardioembolic IIS among patients with low ejection fraction in sinus rhythm. This is supported by trends to lower frequencies of severe IIS and possible cardioembolic IIS in patients on warfarin compared to aspirin.
Copyright © 2013 S. Karger AG, Basel.
Figures
References
-
- Pullicino P, Homma S, Thompson JLP, Freudenberger RS, Sacco RL, Mohr JP. Oral anticoagulation in patients with cardiomyopathy or heart failure in sinus rhythm. Cerebrovasc Dis. 2008;26:322–327. - PubMed
-
- Gibbs CR, Blann AD, Watson RD, Lip GY. Abnormalities of hemorheological, endothelial, and platelet function in patients with chronic heart failure in sinus rhythm: effects of angiotensin-converting enzyme inhibitor and beta-blocker therapy. Circulation. 2001;103:1746–1751. - PubMed
-
- Gottdiener JS, Gay JA, Van Voorhees L, Di Bianco R, Fletcher RD. Frequency and embolic potential of left ventricular thrombus in dilated cardiomyopathy: assessment by 2-dimensional echocardiography. Am J Cardiol. 1983;52:1281–1285. - PubMed
-
- Pullicino P, Thompson JLP, Barton B, Levin B, Graham S, Freudenberger RS WARCEF Investigators. Warfarin versus Aspirin in Patients with Reduced Cardiac Ejection Fraction (WARCEF): rationale, objectives and design. J Cardiac Fail. 2006;12:39–46. - PubMed
-
- Homma S, Thompson JLP, Pullicino PM, Levin B, Freudenberger RS, Teerlink JR, Ammon SE, Graham S, Sacco RL, Mann DL, Mohr JP, Massie BM, Labovitz AJ, Anker SD, Lok DJ, Ponikowski P, Estol CJ, Lip GY, Di Tullio MR, Sanford AR, Mejia V, Gabriel AP, del Valle ML, Buchsbaum R. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366:1859–1869. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
