

Organ allocation in adults with congenital heart disease listed for heart transplant: impact of ventricular assist devices
- PMID: 23921356
- PMCID: PMC3800508
- DOI: 10.1016/j.healun.2013.06.024
Organ allocation in adults with congenital heart disease listed for heart transplant: impact of ventricular assist devices
Abstract
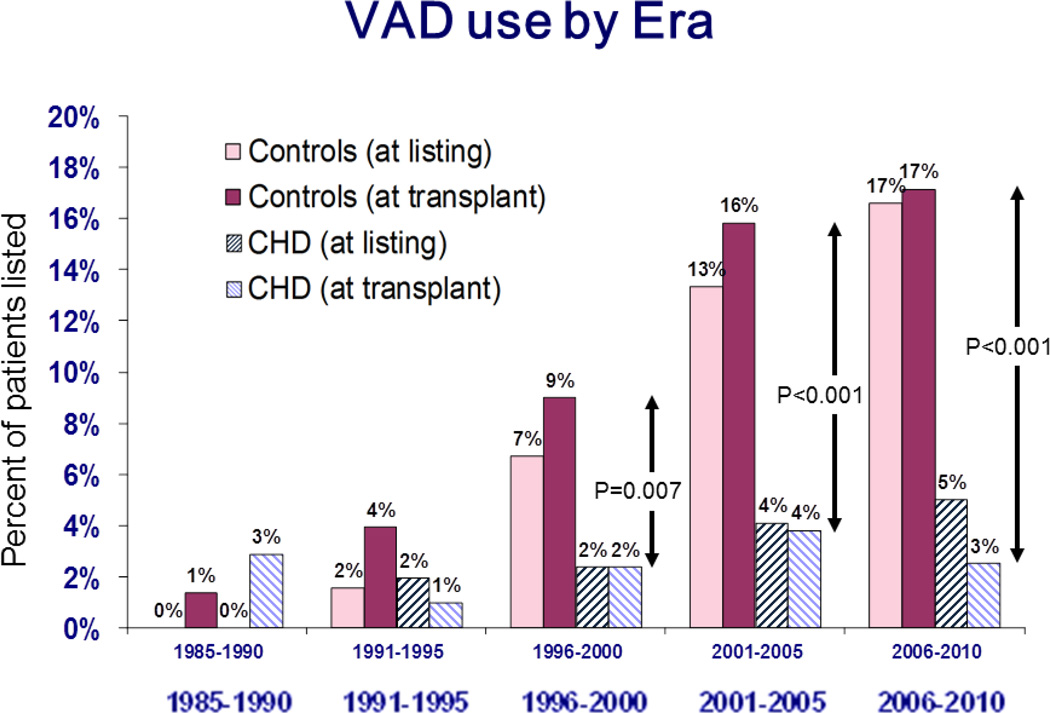
Background: Adults with congenital heart disease (CHD) listed for heart transplantation are rarely supported by ventricular assist devices (VADs). This may be a disadvantage to their priority for organ allocation. We sought to determine the relationship between VAD implantation and successful transplantation among patients listed for heart transplant.
Methods: Adults with CHD patients (N = 1,250) were identified from the United Network for Organ Sharing (UNOS) database from 1985 to 2010 and compared to patients without congenital etiology for heart failure (N = 59,606). VAD use at listing, listing status, status upgrades and reasons for upgrade prior to transplant were trended at 5-year intervals and appropriate statistical comparisons were made between groups.
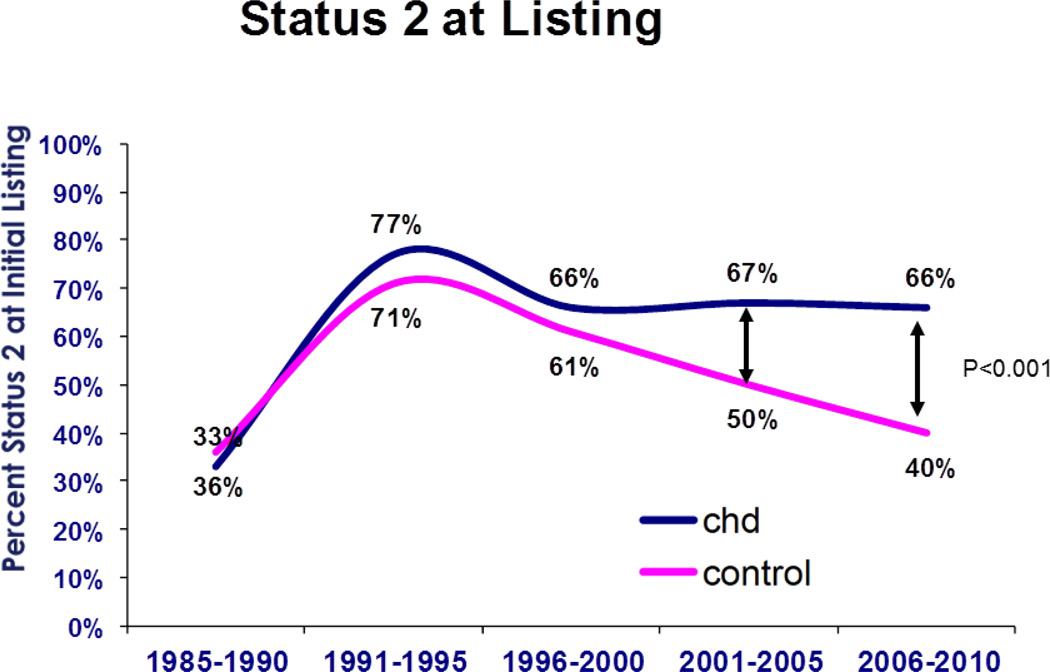
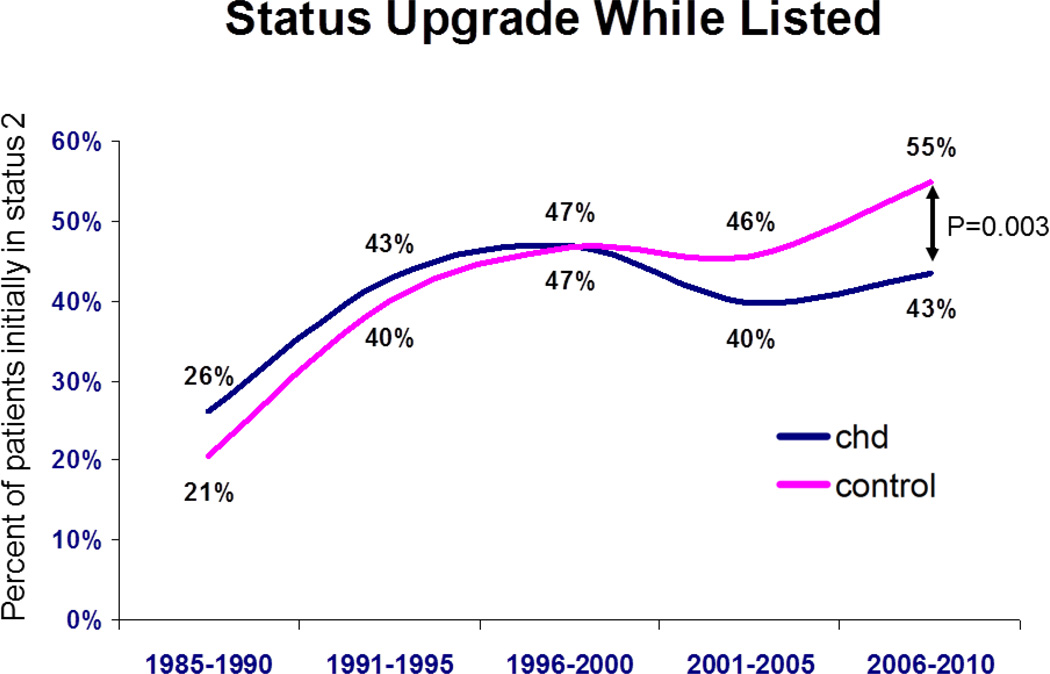
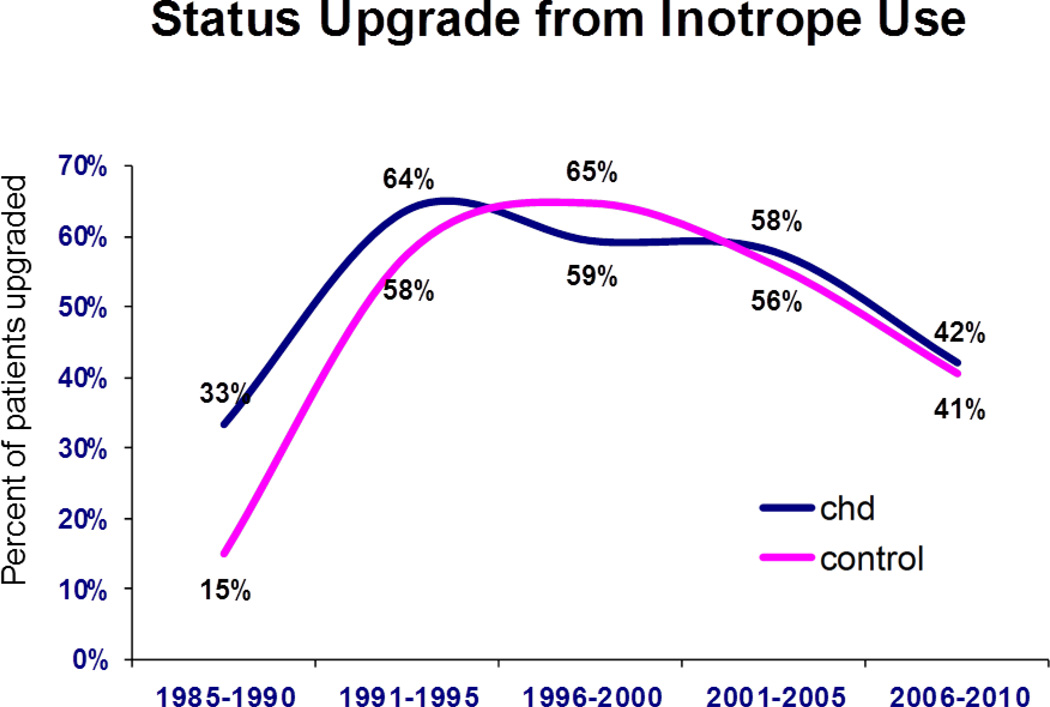
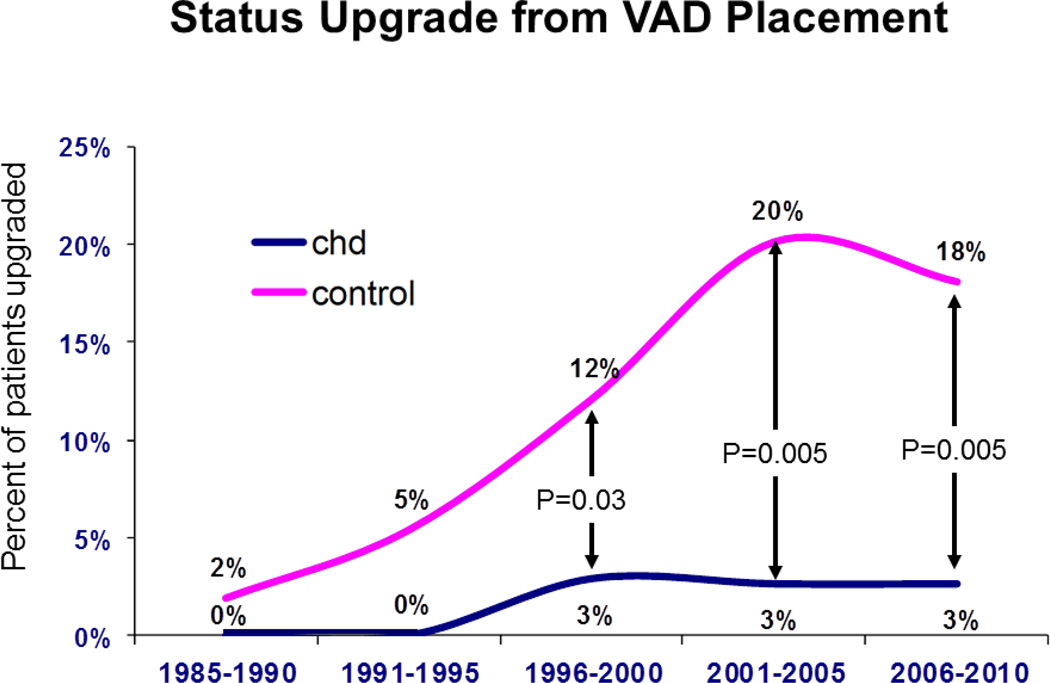
Results: Since 1985, VAD use prior to transplant has increased significantly in patients without CHD, but not in CHD patients (17% vs 3% in 2006 to 2010, p < 0.0001). CHD patients were more likely to be listed as Status 2, compared to those without (66% vs 40%, p < 0.001 for 2006 to 2010), and less likely to be upgraded to Status 1 after listing (43% vs 55%, p = 0.03). Among those upgraded to Status 1, CHD patients were less likely to have a VAD at transplant than those without (3% vs 18%, p = 0.005). VAD use was more likely to result in death in CHD patients.
Conclusions: VAD use is less common in CHD patients than in patients without CHD, both at the time of listing and transplantation. Reduced VAD use appears to contribute to lower listing status and organ allocation. These differences have grown more disparate over time. Separate criteria for organ allocation for CHD patients may be justified.
Keywords: congenital; heart defects; heart failure; heart transplantation; transplant organ allocation; ventricular assist device.
© 2013 International Society for Heart and Lung Transplantation. All rights reserved.
Conflict of interest statement
Conflict of Interest
None of the authors have any relevant financial relationships to disclose.
Figures
Comment in
-
Leveling the playing field in adult heart transplantation.J Heart Lung Transplant. 2013 Nov;32(11):1052-3. doi: 10.1016/j.healun.2013.09.002. J Heart Lung Transplant. 2013. PMID: 24135039 No abstract available.
Similar articles
-
Effects of the 2006 U.S. thoracic organ allocation change: analysis of local impact on organ procurement and heart transplantation.J Heart Lung Transplant. 2010 Mar;29(3):235-9. doi: 10.1016/j.healun.2009.05.036. Epub 2009 Sep 26. J Heart Lung Transplant. 2010. PMID: 19782588
-
Impact of Durable Ventricular Assist Device Support on Outcomes of Patients with Congenital Heart Disease Waiting for Heart Transplant.ASAIO J. 2020 May;66(5):513-519. doi: 10.1097/MAT.0000000000001041. ASAIO J. 2020. PMID: 31335373
-
The change in heart allocation policy in the United States: is it working as designed?J Heart Lung Transplant. 2010 Mar;29(3):255-6. doi: 10.1016/j.healun.2009.09.016. Epub 2009 Dec 24. J Heart Lung Transplant. 2010. PMID: 20036163 No abstract available.
-
Outcomes of Children Supported With Pulsatile Paracorporeal Ventricular Assist Device: Congenital Versus Acquired Heart Disease.World J Pediatr Congenit Heart Surg. 2023 Nov;14(6):708-715. doi: 10.1177/21501351231181105. Epub 2023 Aug 23. World J Pediatr Congenit Heart Surg. 2023. PMID: 37609822 Review.
-
Ventricular assist device use in congenital heart disease with a comparison to heart transplant.J Comp Eff Res. 2014 Sep;3(5):533-46. doi: 10.2217/cer.14.42. J Comp Eff Res. 2014. PMID: 25350804 Free PMC article. Review.
Cited by
-
Considerations for patients awaiting heart transplantation-Insights from the UK experience.J Thorac Dis. 2015 Mar;7(3):527-31. doi: 10.3978/j.issn.2072-1439.2015.01.07. J Thorac Dis. 2015. PMID: 25922735 Free PMC article.
-
Heart failure in systemic right ventricle: Mechanisms and therapeutic options.Front Cardiovasc Med. 2023 Jan 10;9:1064196. doi: 10.3389/fcvm.2022.1064196. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36704462 Free PMC article. Review.
-
Surgical outcomes in complex adult congenital heart disease: a brief review.J Thorac Dis. 2020 Mar;12(3):1224-1234. doi: 10.21037/jtd.2019.12.136. J Thorac Dis. 2020. PMID: 32274204 Free PMC article. Review.
-
The Miracle Baby Grows Up: Hypoplastic Left Heart Syndrome in the Adult.Curr Cardiol Rep. 2017 Aug;19(8):74. doi: 10.1007/s11886-017-0877-3. Curr Cardiol Rep. 2017. PMID: 28744764 Review.
-
Mechanical support for the failing single ventricle after Fontan.JTCVS Tech. 2022 Feb 15;13:174-181. doi: 10.1016/j.xjtc.2021.12.019. eCollection 2022 Jun. JTCVS Tech. 2022. PMID: 35713590 Free PMC article. No abstract available.
References
-
- Bolger AP, Coats AJ, Gatzoulis MA. Congenital heart disease: The original heart failure syndrome. Eur Heart J. 2003;24:970–976. - PubMed
-
- Nieminen HP, Jokinen EV, Sairanen HI. Causes of late deaths after pediatric cardiac surgery: A population-based study. J Am Coll Cardiol. 2007;50:1263–1271. - PubMed
-
- Oechslin EN, Harrison DA, Connelly MS, Webb GD, Siu SC. Mode of death in adults with congenital heart disease. Am J Cardiol. 2000;86:1111–1116. - PubMed
-
- Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dobbels F, Kirk R, Rahmel AO, Hertz MI. The registry of the international society for heart and lung transplantation: Twenty-eighth adult heart transplant report-2011. J Heart Lung Transplant. 2011;30:1078–1094. - PubMed
-
- Hosseinpour AR, Cullen S, Tsang VT. Transplantation for adults with congenital heart disease. Eur J Cardiothorac Surg. 2006;30:508–514. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
