

Hepatic arterial infusion chemotherapy in hepatocellular carcinoma with portal vein tumor thrombosis
- PMID: 23922465
- PMCID: PMC3732840
- DOI: 10.3748/wjg.v19.i29.4679
Hepatic arterial infusion chemotherapy in hepatocellular carcinoma with portal vein tumor thrombosis
Abstract
Aim: To evaluate the prognostic factors and efficacy of hepatic arterial infusion chemotherapy in hepatocellular carcinoma with portal vein tumor thrombosis.
Methods: Fifty hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT) were treated using hepatic arterial infusion chemotherapy (HAIC) via a subcutaneously implanted port. The epirubicin-cisplatin-5-fluorouracil (ECF) chemotherapeutic regimen consisted of 35 mg/m(2) epirubicin on day 1, 60 mg/m(2) cisplatin for 2 h on day 2, and 500 mg/m(2) 5-fluorouracil for 5 h on days 1-3. The treatments were repeated every 3 or 4 wk.
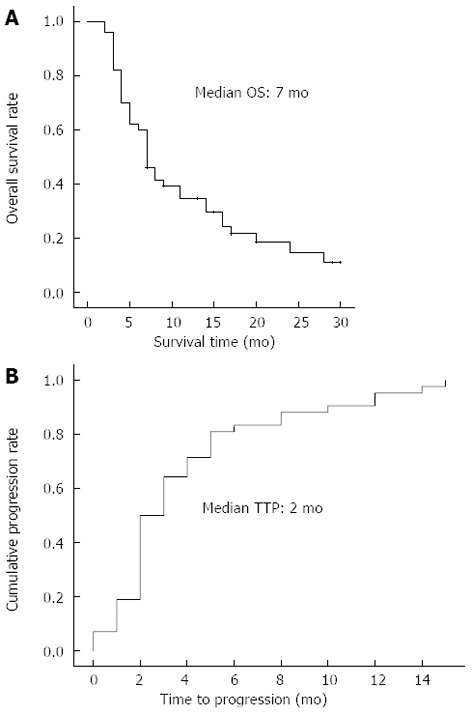
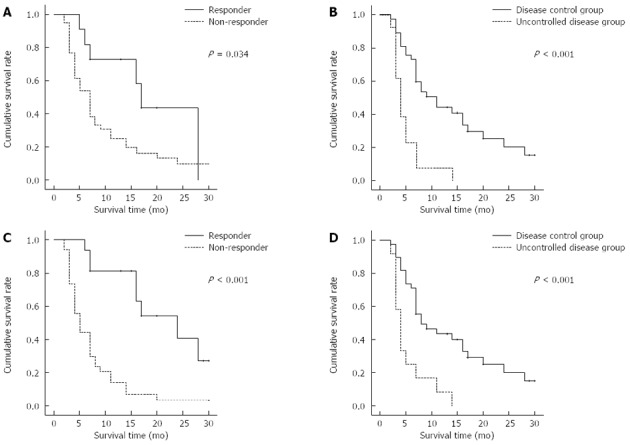
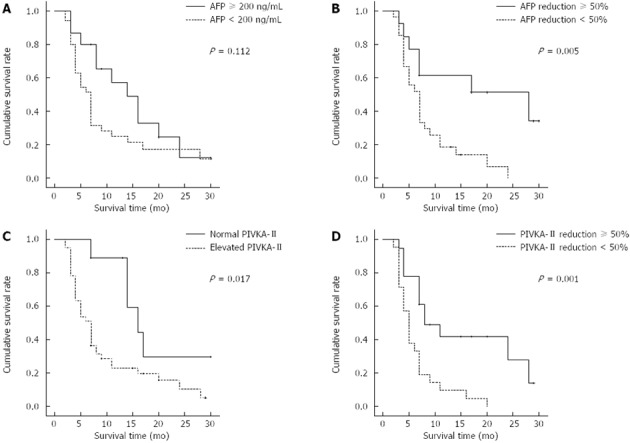
Results: Three (6%) of the 50 patients achieved a complete response (CR), 13 (26%) showed partial responses (PR), and 22 (44%) had stable disease (SD). The median survival and time to progression were 7 and 2 mo, respectively. After 2 cycles of HAIC, CR was achieved in 1 patient (2%), PR in 10 patients (20%) and SD in 26 patients (52%). Significant pre-treatment prognostic factors were a tumor volume of < 400 cm(3) (P = 0.01) and normal levels of protein induced by vitamin K absence or antagonist (PIVKA)-II (P = 0.022). After 2 cycles of treatment, disease control (CR + PR + SD) (P = 0.001), PVTT response (P = 0.003) and α-fetoprotein reduction of over 50% (P = 0.02) were independent factors for survival. Objective response (CR + PR), disease control, PVTT response, and combination therapy during the HAIC were also significant prognostic factors. Adverse events were tolerable and successfully managed.
Conclusion: HAIC may be an effective treatment modality for advanced HCC with PVTT in patients with tumors < 400 cm(3) and good prognostic factors.
Keywords: Hepatic arterial infusion chemotherapy; Hepatocellular carcinoma; Portal vein tumor thrombosis.
Figures
Similar articles
-
Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis: analysis of 48 cases.Cancer. 2002 Aug 1;95(3):588-95. doi: 10.1002/cncr.10694. Cancer. 2002. PMID: 12209752 Clinical Trial.
-
A comparative study between sorafenib and hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis.J Gastroenterol. 2015 Apr;50(4):445-54. doi: 10.1007/s00535-014-0978-3. Epub 2014 Jul 16. J Gastroenterol. 2015. PMID: 25027973
-
Improved survival for hepatocellular carcinoma with portal vein tumor thrombosis treated by intra-arterial chemotherapy combining etoposide, carboplatin, epirubicin and pharmacokinetic modulating chemotherapy by 5-FU and enteric-coated tegafur/uracil: a pilot study.World J Gastroenterol. 2007 Nov 7;13(41):5465-70. doi: 10.3748/wjg.v13.i41.5465. World J Gastroenterol. 2007. PMID: 17907289 Free PMC article. Clinical Trial.
-
Systematic review of hepatic arterial infusion chemotherapy versus sorafenib in patients with hepatocellular carcinoma with portal vein tumor thrombosis.J Gastroenterol Hepatol. 2020 Aug;35(8):1277-1287. doi: 10.1111/jgh.15010. Epub 2020 Mar 3. J Gastroenterol Hepatol. 2020. PMID: 32052876
-
Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus.World J Gastroenterol. 2006 Dec 21;12(47):7561-7. doi: 10.3748/wjg.v12.i47.7561. World J Gastroenterol. 2006. PMID: 17171782 Free PMC article. Review.
Cited by
-
Lung metastases after liver cancer resection cured by immunotherapy: case report and literature review.Anticancer Drugs. 2023 Jan 1;34(1):e1-e8. doi: 10.1097/CAD.0000000000001371. Epub 2022 Sep 5. Anticancer Drugs. 2023. PMID: 36066392 Free PMC article. Review.
-
The Role of Ferroptosis in the Treatment and Drug Resistance of Hepatocellular Carcinoma.Front Cell Dev Biol. 2022 Mar 3;10:845232. doi: 10.3389/fcell.2022.845232. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 35309918 Free PMC article. Review.
-
Role and limitation of neoadjuvant hepatic arterial infusion chemotherapy in advanced hepatocelluar carcinoma patients with Child-Pugh class A.World J Surg Oncol. 2019 Aug 15;17(1):143. doi: 10.1186/s12957-019-1685-6. World J Surg Oncol. 2019. PMID: 31416447 Free PMC article.
-
Hepatic Arterial Infusion Chemotherapy Followed by Lipiodol Infusion for Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: A Single-Center Experience.Medicina (Kaunas). 2021 Jul 30;57(8):779. doi: 10.3390/medicina57080779. Medicina (Kaunas). 2021. PMID: 34440985 Free PMC article.
-
Hepatic arterial infusion chemotherapy for patients with huge unresectable hepatocellular carcinoma.PLoS One. 2014 May 13;9(5):e92784. doi: 10.1371/journal.pone.0092784. eCollection 2014. PLoS One. 2014. PMID: 24824520 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Sangiovanni A, Del Ninno E, Fasani P, De Fazio C, Ronchi G, Romeo R, Morabito A, De Franchis R, Colombo M. Increased survival of cirrhotic patients with a hepatocellular carcinoma detected during surveillance. Gastroenterology. 2004;126:1005–1014. - PubMed
-
- Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology. 2003;37:429–442. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–390. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
