

Clinical outcome in patients with hepatocellular carcinoma after living-donor liver transplantation
- PMID: 23922471
- PMCID: PMC3732846
- DOI: 10.3748/wjg.v19.i29.4737
Clinical outcome in patients with hepatocellular carcinoma after living-donor liver transplantation
Abstract
Aim: To investigate risk factors for hepatocellular carcinoma (HCC) recurrence after living donor liver transplantation (LDLT) and efficacy of various criteria.
Methods: From October 2000 to November 2011, 233 adult patients underwent LDLT for HCC at our institution. After excluding nine postoperative mortality cases, we analyzed retrospectively 224 patients. To identify risk factors for recurrence, we evaluated recurrence, disease-free survival (DFS) rate, survival rate, and various other factors which are based on the characteristics of both the patient and tumor. Additionally, we developed our own criteria based on our data. Next, we compared our selection criteria with various tumor-grading scales, such as the Milan criteria, University of California, San Francisco (UCSF) criteria, TNM stage, Barcelona Clinic Liver Cancer (BCLC) stage and Cancer of the Liver Italian Program (CLIP) scoring system. The median follow up was 68 (6-139) mo.
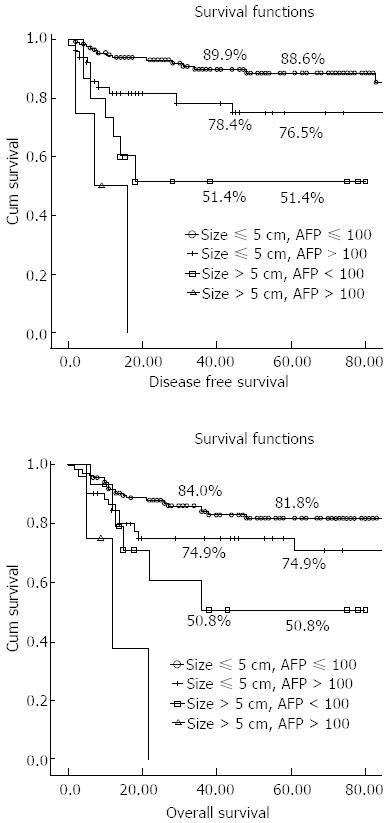
Results: In 224 patients who received LDLT for HCC, 37 (16.5%) experienced tumor recurrence during the follow-up period. The 5-year DFS and overall survival rates after LDLT in all patients with HCC were 80.9% and 76.4%, respectively. On multivariate analysis, the tumor diameter {5 cm; P < 0.001; exponentiation of the B coefficient [Exp(B)], 11.89; 95%CI: 3.784-37.368} and alpha fetoprotein level [AFP, 100 ng/mL; P = 0.021; Exp(B), 2.892; 95%CI: 1.172-7.132] had significant influences on HCC recurrence after LDLT. Therefore, these two factors were included in our criteria. Based on these data, we set our selection criteria as a tumor diameter ≤ 5 cm and AFP ≤ 100 ng/mL. Within our new criteria (140/214, 65.4%), the 5-year DFS and overall survival rates were 88.6% and 81.8%, respectively. Our criteria (P = 0.001), Milan criteria (P = 0.009), and UCSF criteria (P = 0.001) showed a significant difference in DFS rate. And our criteria (P = 0.006) and UCSF criteria (P = 0.009) showed a significant difference in overall survival rate. But Milan criteria did not show significant difference in overall survival rate (P = 0.137). Among stages 0, A, B and C of BCLC, stage C had a significantly higher recurrence rate (P = 0.001), lower DFS (P = 0.001), and overall survival rate (P = 0.005) compared with the other stages. Using the CLIP scoring system, the group with a score of 4 to 5 showed a high recurrence rate (P = 0.023) and lower DFS (P = 0.011); however, the overall survival rate did not differ from that of the lower scoring group. The TNM system showed a trend of increased recurrence rate, decreased DFS, or survival rate according to T stage, albeit without statistical significance.
Conclusion: LDLT is considered the preferred therapeutic option in patients with an AFP level less than 100 ng/mL and a tumor diameter of less than 5 cm.
Keywords: Barcelona Clinic Liver Cancer; Cancer of the Liver Italian Program; Hepatocellular carcinoma; Living donor liver transplantation; Milan criteria; Selection criteria; University of California, San Francisco criteria.
Figures
References
-
- Ringe B, Pichlmayr R, Wittekind C, Tusch G. Surgical treatment of hepatocellular carcinoma: experience with liver resection and transplantation in 198 patients. World J Surg. 1991;15:270–285. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, Montalto F, Ammatuna M, Morabito A, Gennari L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
-
- Stuart KE, Anand AJ, Jenkins RL. Hepatocellular carcinoma in the United States. Prognostic features, treatment outcome, and survival. Cancer. 1996;77:2217–2222. - PubMed
-
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection vs transplantation. Hepatology. 1999;30:1434–1440. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
