

Association of bronchoalveolar lavage yield with chest computed tomography findings and symptoms in immunocompromised patients
- PMID: 23922610
- PMCID: PMC3731857
- DOI: 10.4103/1817-1737.114302
Association of bronchoalveolar lavage yield with chest computed tomography findings and symptoms in immunocompromised patients
Abstract
Introduction: Fiber-optic bronchoscopy (FOB) with bronchoalveolar lavage (BAL) is a common procedure performed in immunocompromised patients with undiagnosed pulmonary pathology. Identifying patients with the highest potential diagnostic yield may help to avoid morbidity in patients unlikely to benefit from the procedure. We sought to determine which patient factors, specifically chest computed tomography (CT) findings, affected diagnostic yield of BAL.
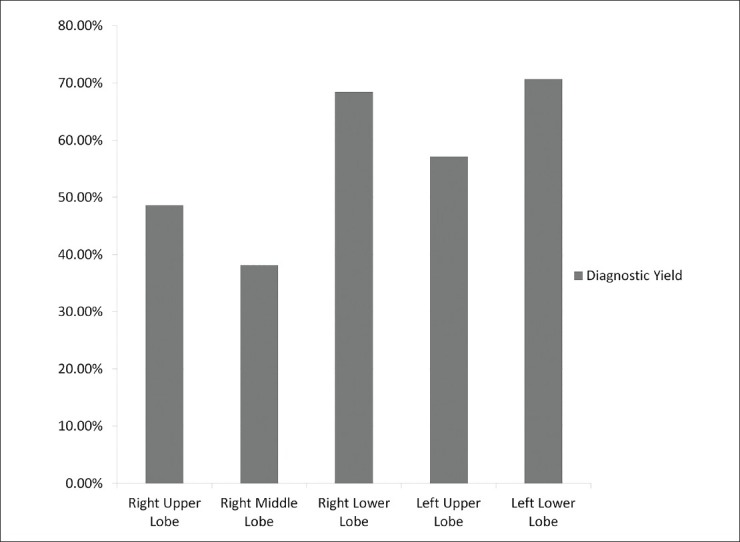
Methods: Retrospective chart review of immunocompromised patients who underwent FOB with BAL from 01/01/2010 to 12/31/2011 at an academic medical center was performed. The lung lobe lavaged, characteristics of pulmonary infiltrate on radiograph, patient symptoms, and diagnostic yield were collected. A positive diagnostic yield was defined as a positive microbiological culture, finding on cytopathologic staining, diffuse alveolar hemorrhage, alveolar eosinophilia or a positive immunologic or nucleic acid assay.
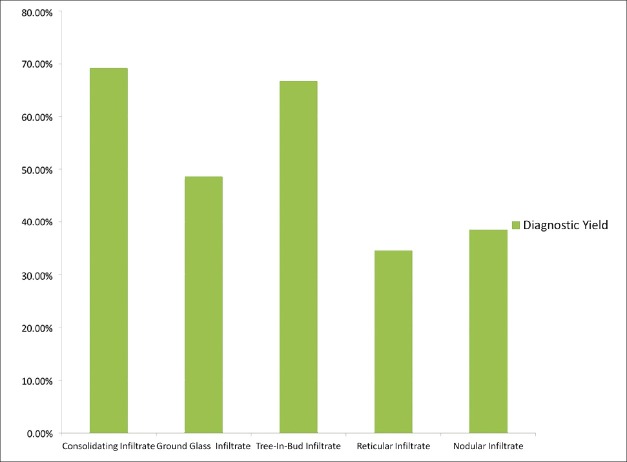
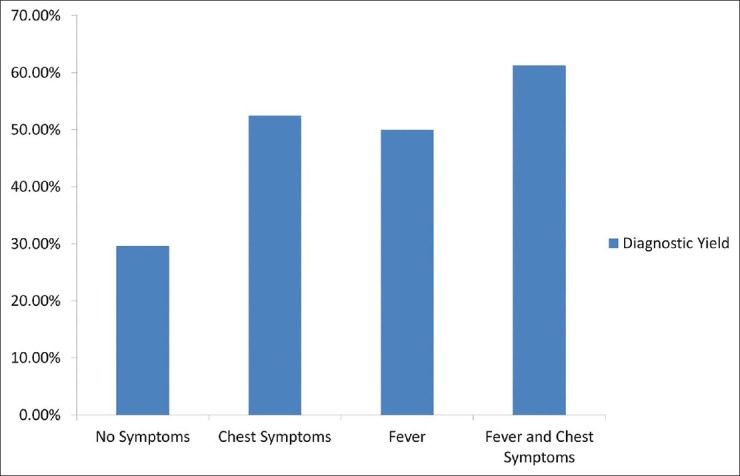
Results: The overall diagnostic yield was 52.6%. Infiltrates that were predominantly reticular or nodular by CT had a lower diagnostic yield than predominantly consolidated, ground-glass, or tree-in-bud infiltrates (36.5% vs. 61.2%, P = 0.0058). The diagnostic yield was significantly improved in patients with both fever and chest symptoms compared to patients without symptoms (61.3% vs. 29.6%, P = 0.0066).
Conclusion: CT findings of reticular and nodular infiltrates portend a worse diagnostic yield from BAL than those that are alveolar in nature. Symptomatic patients are more likely to have diagnostic FOB with BAL than asymptomatic patients.
Keywords: Bronchoscopy; computed tomography; immunodeficiency; respiratory infection; respiratory symptoms.
Conflict of interest statement
Figures
References
-
- Azoulay E, Mokart D, Lambert J, Lemiale V, Rabbat A, Kouatchet A, et al. Diagnostic strategy for hematology and oncology patients with acute respiratory failure: Randomized controlled trial. Am J Respir Crit Care Med. 2010;182:1038–46. - PubMed
-
- Gruson D, Hilbert G, Valentino R, Vargas F, Chene G, Bebear C, et al. Utility of fiberoptic bronchoscopy in neutropenic patients admitted to the intensive care unit with pulmonary infiltrates. Crit Care Med. 2000;28:2224–30. - PubMed
-
- Hohenthal U, Itälä M, Salonen J, Sipilä J, Rantakokko-Jalava K, Meurman O, et al. Bronchoalveolar lavage in immunocompromised patients with haematological malignancy: Value of new microbiological methods. Eur J Haematol. 2005;74:203–11. - PubMed
-
- Joos L, Chhajed PN, Wallner J, Battegay M, Steiger J, Gratwohl A, et al. Pulmonary infections diagnosed by BAL: A 12-year experience in 1066 immunocompromised patients. Respir Med. 2007;101:93–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
