

The epidemiological modelling of major depressive disorder: application for the Global Burden of Disease Study 2010
- PMID: 23922765
- PMCID: PMC3726670
- DOI: 10.1371/journal.pone.0069637
The epidemiological modelling of major depressive disorder: application for the Global Burden of Disease Study 2010
Abstract
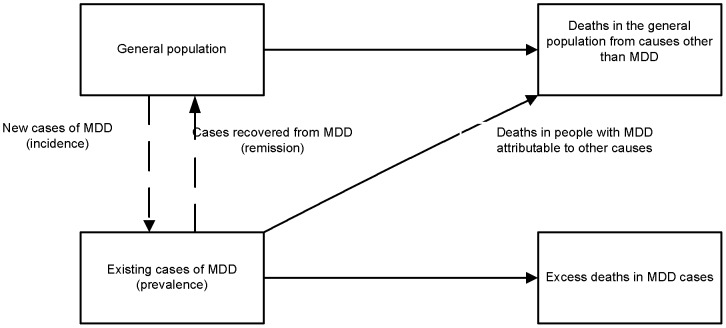
Background: Although the detrimental impact of major depressive disorder (MDD) at the individual level has been described, its global epidemiology remains unclear given limitations in the data. Here we present the modelled epidemiological profile of MDD dealing with heterogeneity in the data, enforcing internal consistency between epidemiological parameters and making estimates for world regions with no empirical data. These estimates were used to quantify the burden of MDD for the Global Burden of Disease Study 2010 (GBD 2010).
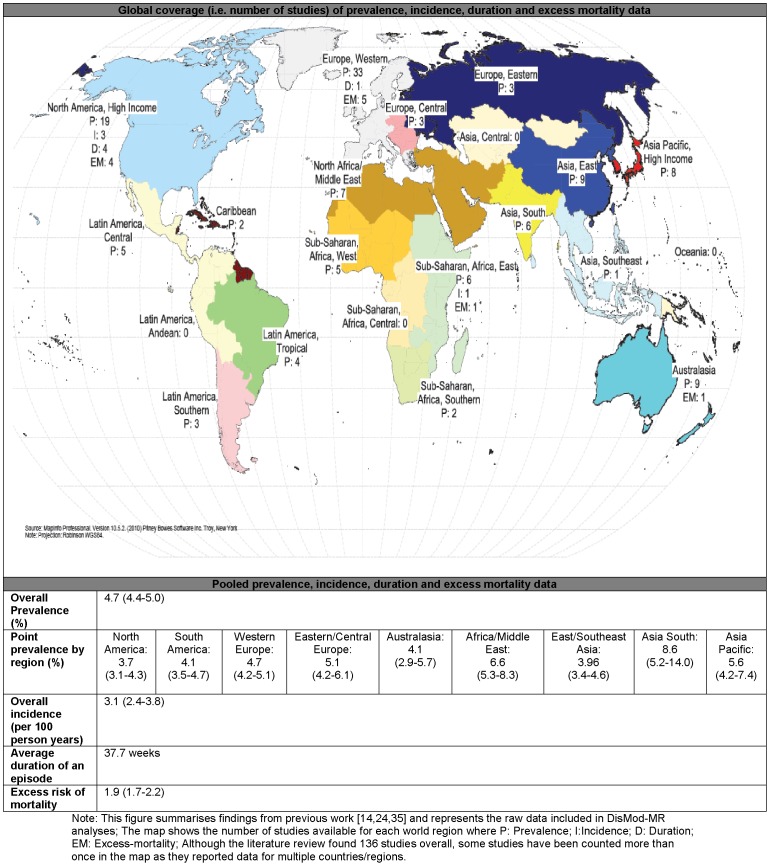
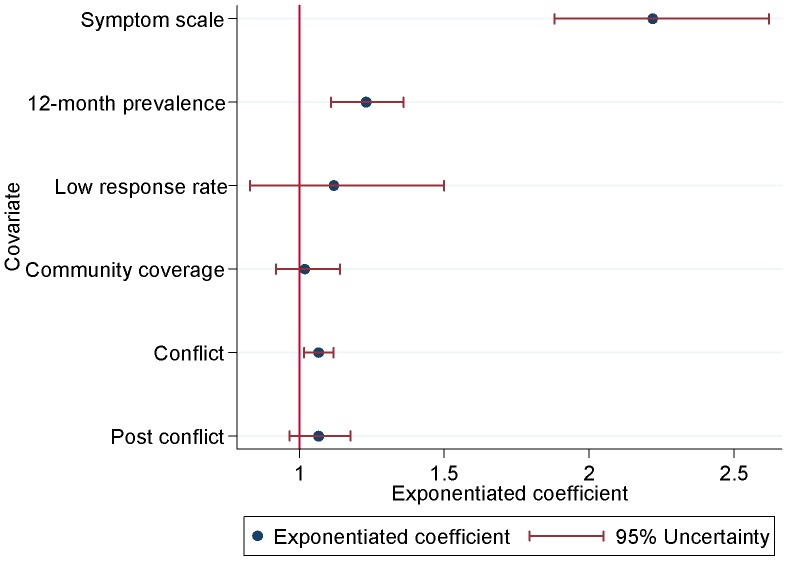
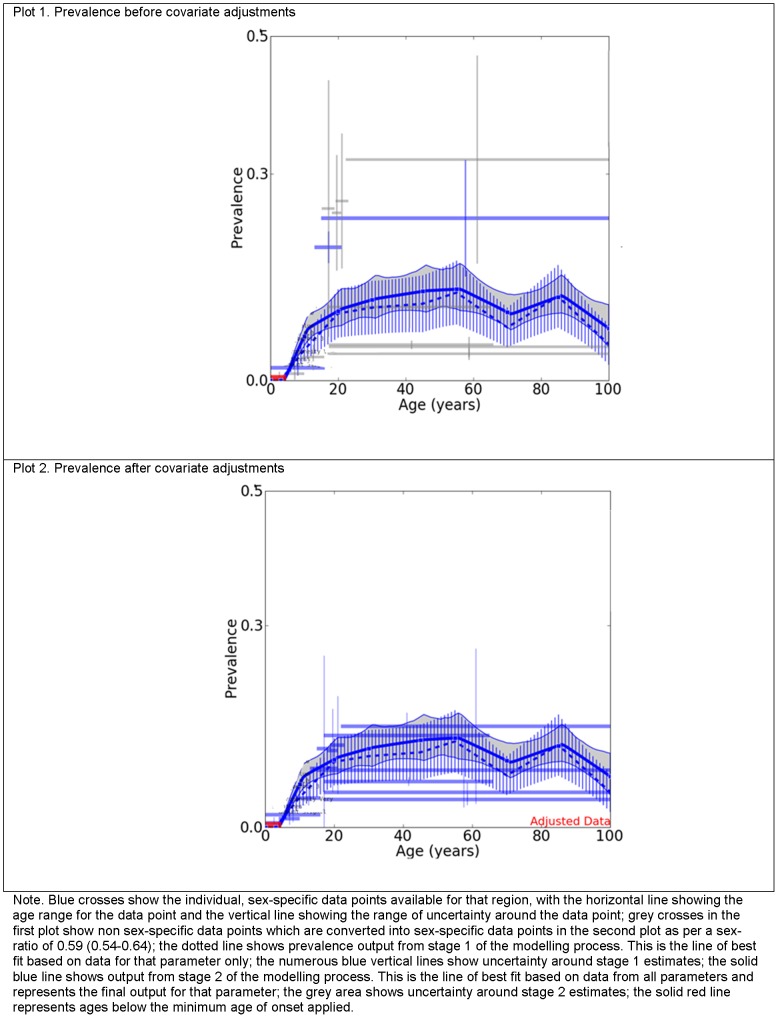
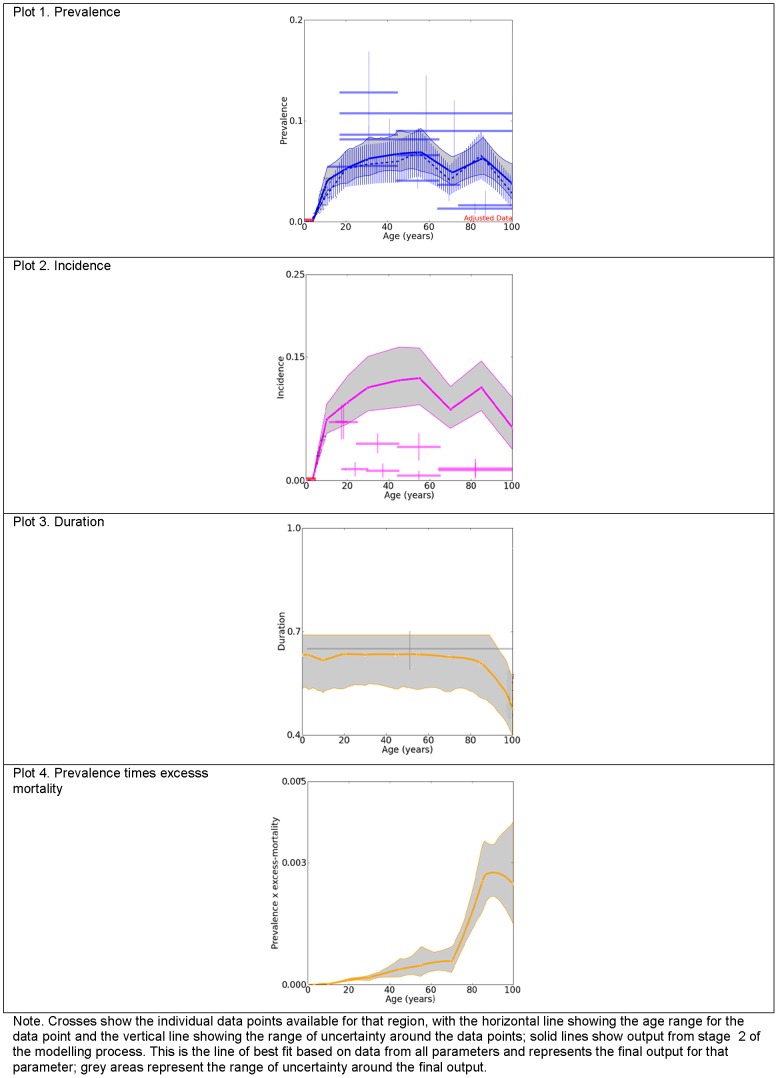
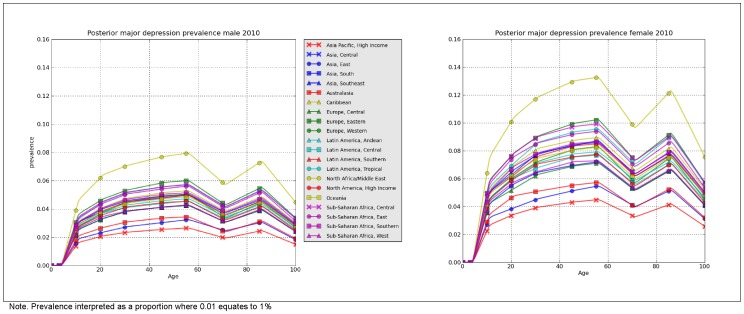
Method: Analyses drew on data from our existing literature review of the epidemiology of MDD. DisMod-MR, the latest version of the generic disease modelling system redesigned as a Bayesian meta-regression tool, derived prevalence by age, year and sex for 21 regions. Prior epidemiological knowledge, study- and country-level covariates adjusted sub-optimal raw data.
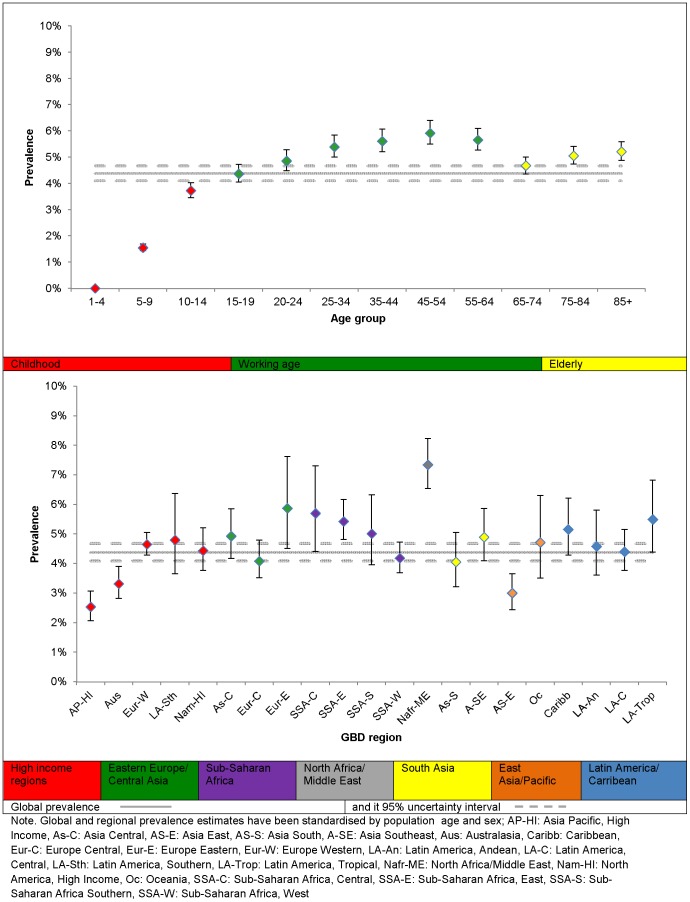
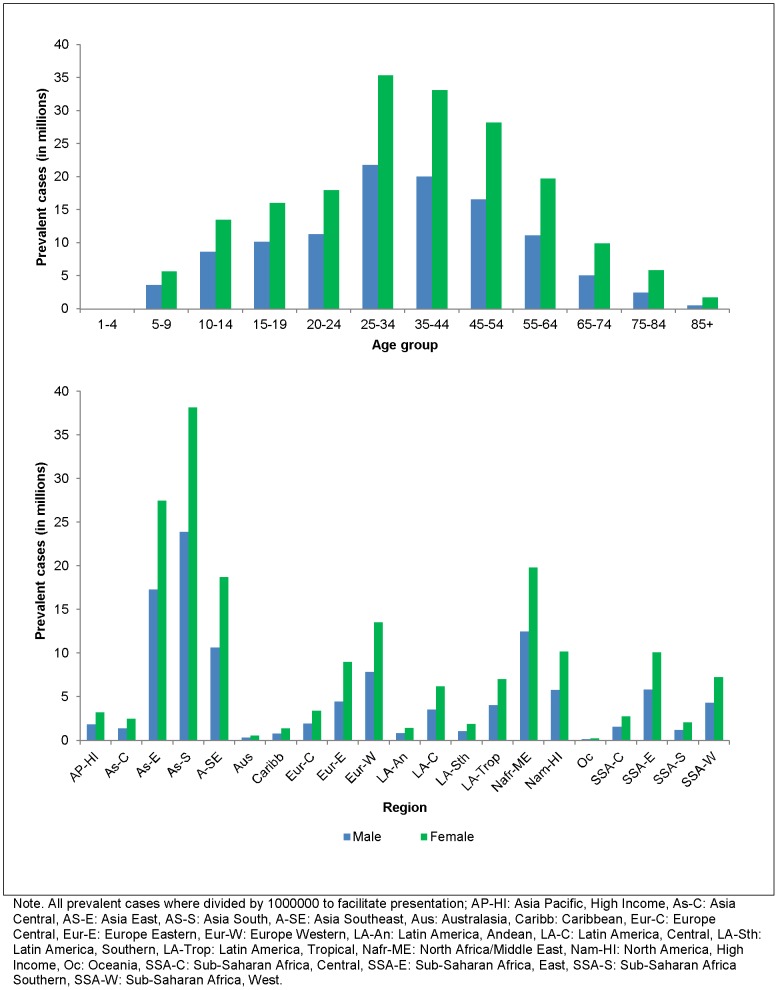
Results: There were over 298 million cases of MDD globally at any point in time in 2010, with the highest proportion of cases occurring between 25 and 34 years. Global point prevalence was very similar across time (4.4% (95% uncertainty: 4.2-4.7%) in 1990, 4.4% (4.1-4.7%) in 2005 and 2010), but higher in females (5.5% (5.0-6.0%) compared to males (3.2% (3.0-3.6%) in 2010. Regions in conflict had higher prevalence than those with no conflict. The annual incidence of an episode of MDD followed a similar age and regional pattern to prevalence but was about one and a half times higher, consistent with an average duration of 37.7 weeks.
Conclusion: We were able to integrate available data, including those from high quality surveys and sub-optimal studies, into a model adjusting for known methodological sources of heterogeneity. We were also able to estimate the epidemiology of MDD in regions with no available data. This informed GBD 2010 and the public health field, with a clearer understanding of the global distribution of MDD.
Conflict of interest statement
Figures
References
-
- Kessler RC (1999) The World Health Organization International Consortium in Psychiatric Epidemiology (ICPE): initial work and future directions – the NAPE Lecture 1998. Nordic Association for Psychiatric Epidemiology. Acta Psychiatr Scand 99: 2–9. - PubMed
-
- Skapinakis P, Lewis G (2001) Epidemiology in community psychiatric research: common uses and methodological issues. Epidemiol Psichiatr Soc 10: 18–26. - PubMed
-
- Wittchen HU (2000) Epidemiological research in mental disorders: lessons for the next decade of research–the NAPE Lecture 1999. Nordic Association for Psychiatric Epidemiology. Acta Psychiatr Scand 101: 2–10. - PubMed
-
- Murray CJL, Lopez AD, editors(1996) The Global Burden of Disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. USA: World Health Organization, Harvard School of Public Health, World Bank.
-
- World Health Organization (2008) The Global Burden of Disease: 2004 update. Switzerland.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
