

Aliskiren and amlodipine in the management of essential hypertension: meta-analysis of randomized controlled trials
- PMID: 23922924
- PMCID: PMC3726495
- DOI: 10.1371/journal.pone.0070111
Aliskiren and amlodipine in the management of essential hypertension: meta-analysis of randomized controlled trials
Abstract
Background: Aliskiren is a novel renin-angiotensin aldosterone system (RAAS) inhibitor, the combination therapy of aliskiren and amlodipine for blood pressure control have been reported recently. The primary objective of this analysis is to review recently reported randomized controlled trials (RCTs) to compare antihypertensive effects and adverse events between mono (amlodipine or aliskiren alone) and combination therapy of both medicines.
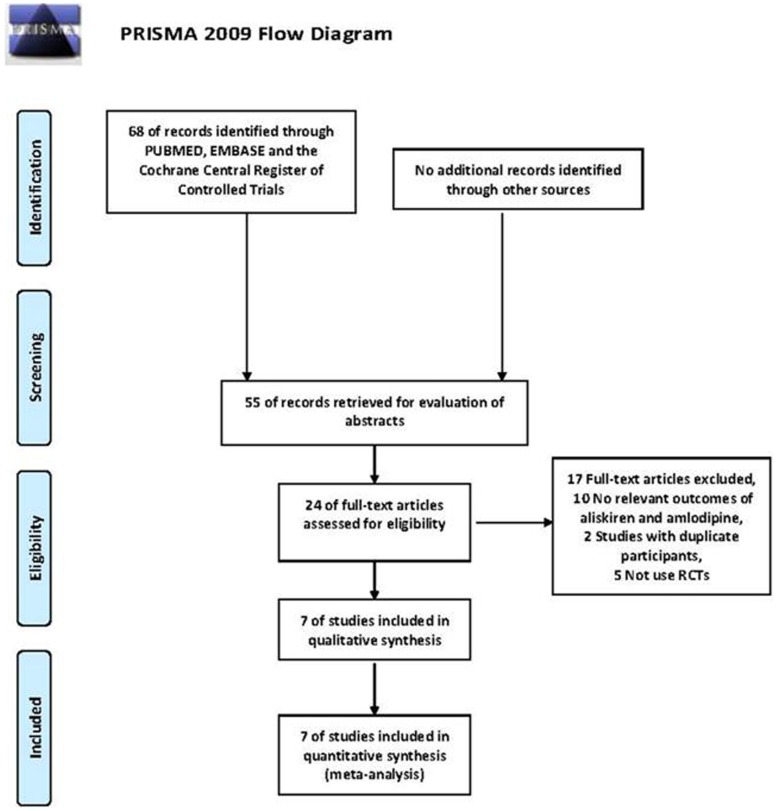
Methods: Databases for the search included Pubmed, Embase and the Cochrane Central Register of Controlled Trials. Revman v5.0 statistical program was used to analyze the data. Weighted mean differences (WMD) with a 95% confidence interval (CI) were used for the calculation of continuous data, and relative risk (RR) with a 95% CI was used for dichotomous data.
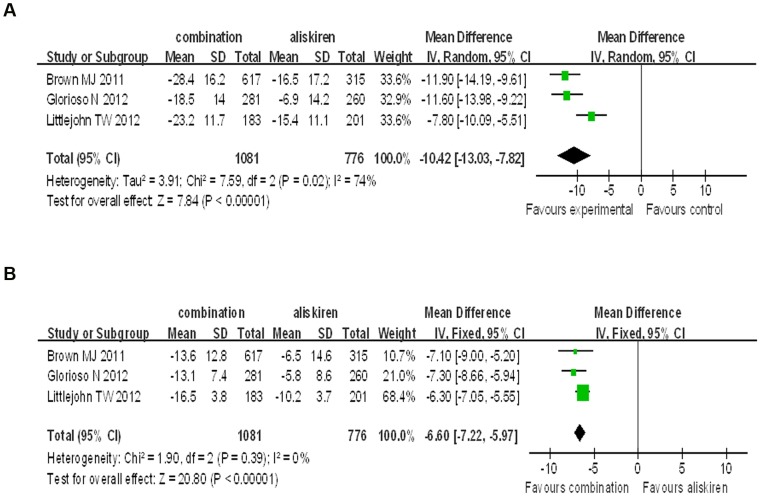
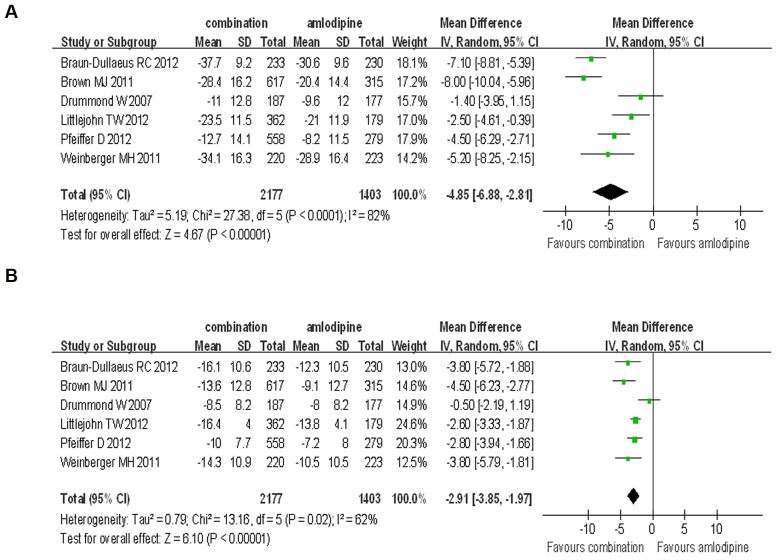
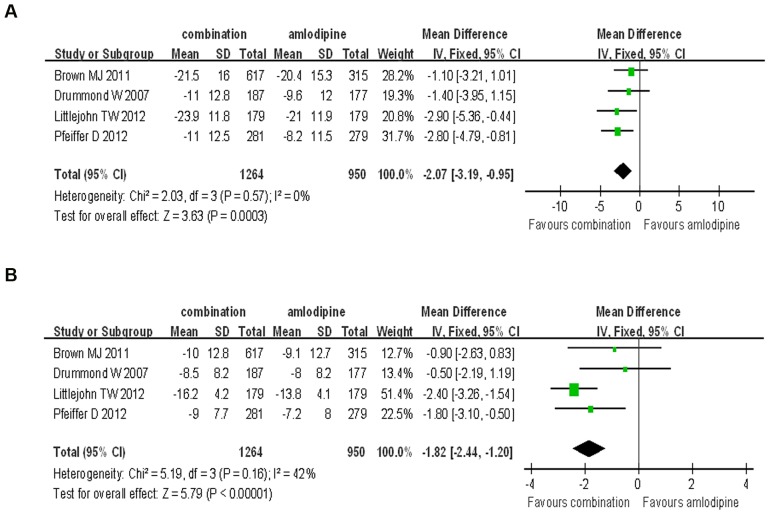
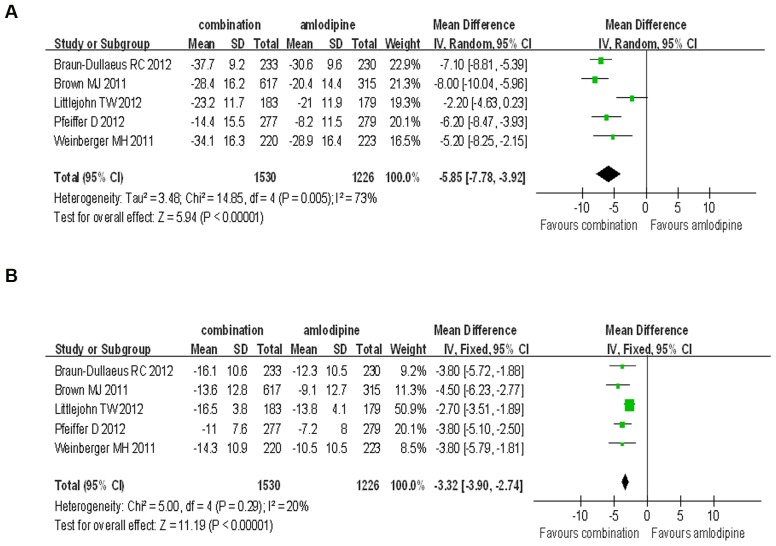
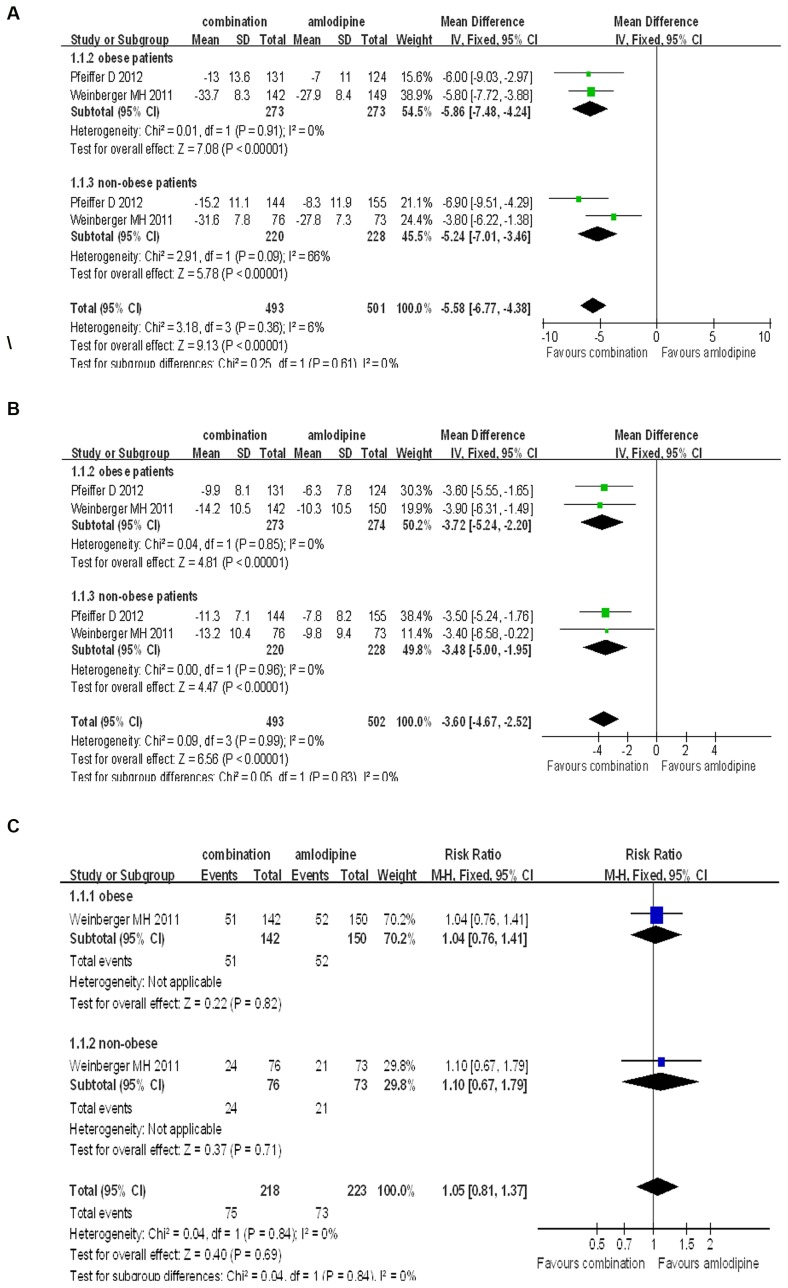
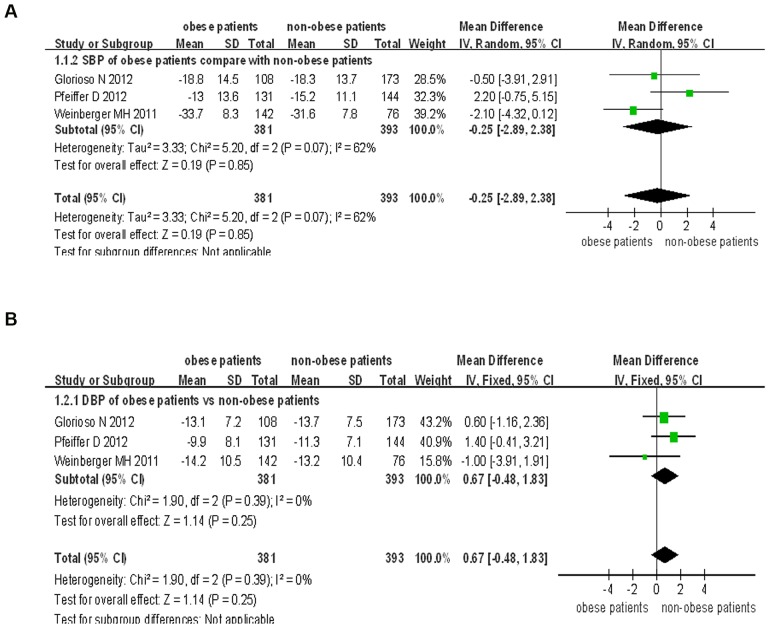
Results: We analyzed the data from 7 RCTs for a total of 6074 participants in this meta-analysis. We found that the aliskiren/amlodipine combination therapy had a stronger effect in lowering blood pressure as compared with the monotherapy using aliskiren (SBP: WMD = -10.42, 95% CI -13.03∼-7.82, P<0.00001; DBP: WMD = -6.60, 95% CI -7.22∼-5.97, P<0.00001) or amlodipine (SBP: WMD = -4.85, 95% CI -6.88∼-2.81, P<0.00001; DBP: WMD = -2.91, 95% CI -3.85∼-1.97, P<0.00001). No differences were found in terms of adverse events between combination therapy and monotherapy, except for the rates of peripheral edema and hypokalaemia which were significantly lower in the combination therapy than in the amlodipine monotherapy (RR = 0.78, 0.66∼0.92, P = 0.004; RR = 0.51, 0.27∼0.97, P = 0.04). Similar antihypertensive effects were found in both obese (body mass index > = 30 kg/m(2)) hypertensive and non-obese (body mass index <30 kg/m(2)) hypertensive patients. Moreover, there was no difference with the blood pressure lowering or adverse effects with regards to the combination therapy in both subgroups.
Conclusion: We found that aliskiren/amlodipine combination therapy provided a more effective blood pressure reduction than monotherapy with either drug without increase in the occurrence of adverse events.
Conflict of interest statement
Figures
References
-
- Wang JG, Staessen JA, Franklin SS, Fagard R, Gueyffier F (2005) Systolic and diastolic blood pressure lowering as determinants of cardiovascular outcome. Hypertension 45: 907–913. - PubMed
-
- Kloner RA, Sowers JR, DiBona GF, Gaffney M, Wein M (1995) Effect of amlodipine on left ventricular mass in the Amlodipine Cardiovascular Community Trial. J Cardiovasc Pharmacol 26: 471–476. - PubMed
-
- Probstfield JL, O'Brien KD (2010) Progression of cardiovascular damage: the role of renin-angiotensin system blockade. Am J Cardiol 105: 10A–20A. - PubMed
-
- Zaman MA, Oparil S, Calhoun DA (2002) Drugs targeting the renin-angiotensin-aldosterone system. Nat Rev Drug Discov 1: 621–636. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
