

Common and rare EGFR and KRAS mutations in a Dutch non-small-cell lung cancer population and their clinical outcome
- PMID: 23922984
- PMCID: PMC3726644
- DOI: 10.1371/journal.pone.0070346
Common and rare EGFR and KRAS mutations in a Dutch non-small-cell lung cancer population and their clinical outcome
Abstract
Introduction: In randomly assigned studies with EGFR TKI only a minor proportion of patients with NSCLC have genetically profiled biopsies. Guidelines provide evidence to perform EGFR and KRAS mutation analysis in non-squamous NSCLC. We explored tumor biopsy quality offered for mutation testing, different mutations distribution, and outcome with EGFR TKI.
Patient and methods: Clinical data from 8 regional hospitals were studied for patient and tumor characteristics, treatment and overall survival. Biopsies sent to the central laboratory were evaluated for DNA quality and subsequently analyzed for mutations in exons 18-21 of EGFR and exon 2 of KRAS by bidirectional sequence analysis.
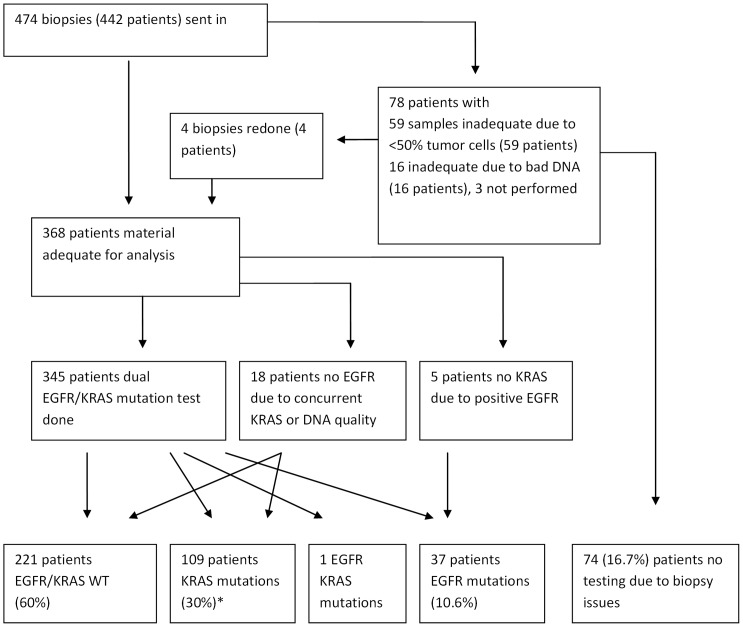
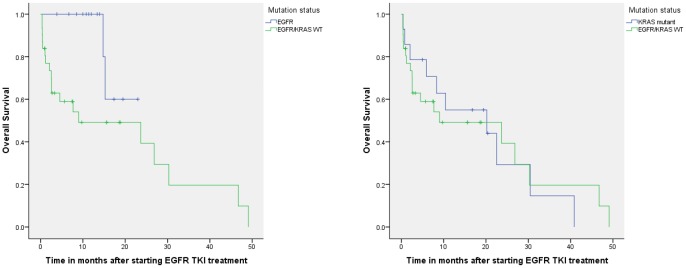
Results: Tumors from 442 subsequent patients were analyzed. For 74 patients (17%) tumors were unsuitable for mutation analysis. Thirty-eight patients (10.9%) had EGFR mutations with 79% known activating mutations. One hundred eight patients (30%) had functional KRAS mutations. The mutation spectrum was comparable to the Cosmic database. Following treatment in the first or second line with EGFR TKI median overall survival for patients with EGFR (n = 14), KRAS (n = 14) mutations and wild type EGFR/KRAS (n = 31) was not reached, 20 and 9 months, respectively.
Conclusion: One out of every 6 tumor samples was inadequate for mutation analysis. Patients with EGFR activating mutations treated with EGFR-TKI have the longest survival.
Conflict of interest statement
Figures
References
-
- Maruyama R, Nishiwaki Y, Tamura T, Yamamoto N, Tsuboi M, et al. (2008) Phase III study, V-15-32, of gefitinib versus docetaxel in previously treated Japanese patients with non-small-cell lung cancer. J Clin Oncol 26: 4244–4252. - PubMed
-
- Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, et al. (2009) Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med 361: 947–957. - PubMed
-
- Douillard JY, Shepherd FA, Hirsh V, Mok T, Socinski MA, et al. (2010) Molecular predictors of outcome with gefitinib and docetaxel in previously treated non-small-cell lung cancer: data from the randomized phase III INTEREST trial. J Clin Oncol 28: 744–752. - PubMed
-
- Ciuleanu T, Stelmakh L, Cicenas S, Miliauskas S, Grigorescu AC, et al. (2012) Efficacy and safety of erlotinib versus chemotherapy in second-line treatment of patients with advanced, non-small-cell lung cancer with poor prognosis (TITAN): a randomised multicentre, open-label, phase 3 study. Lancet Oncol 13: 300–308. - PubMed
-
- Kim ES, Hirsh V, Mok T, Socinski MA, Gervais R, et al. (2008) Gefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised phase III trial. Lancet 372: 1809–1818. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
