

Multiphoton laser tomography and fluorescence lifetime imaging of melanoma: morphologic features and quantitative data for sensitive and specific non-invasive diagnostics
- PMID: 23923016
- PMCID: PMC3724798
- DOI: 10.1371/journal.pone.0070682
Multiphoton laser tomography and fluorescence lifetime imaging of melanoma: morphologic features and quantitative data for sensitive and specific non-invasive diagnostics
Abstract
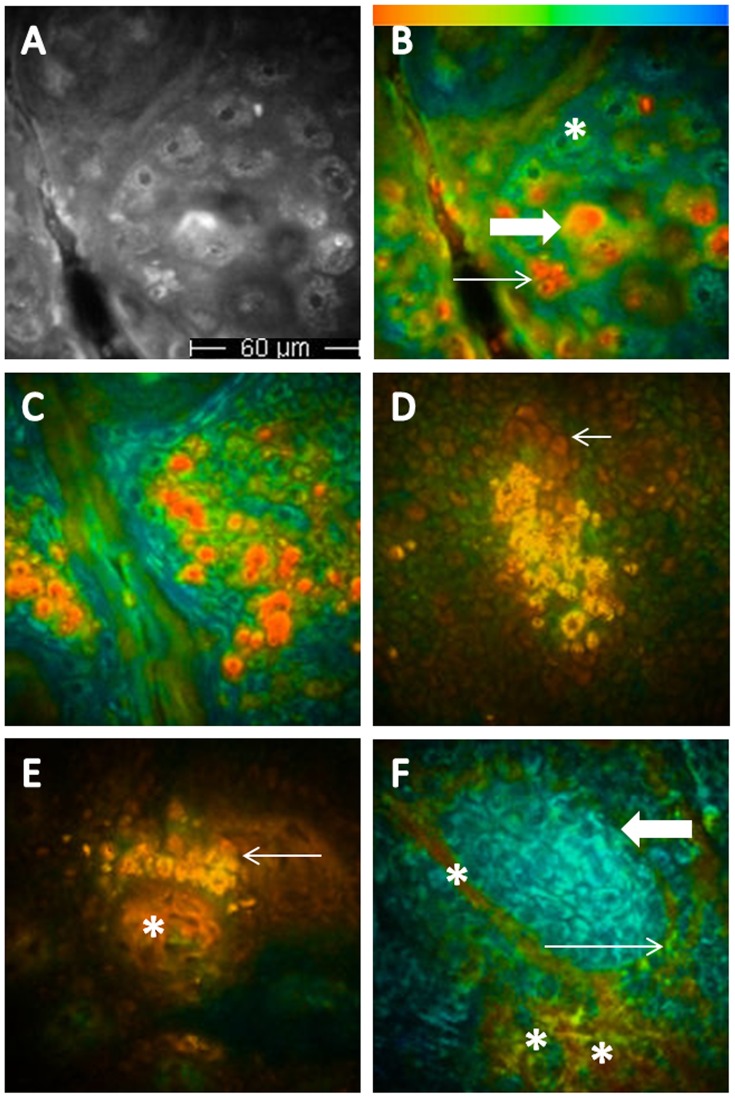
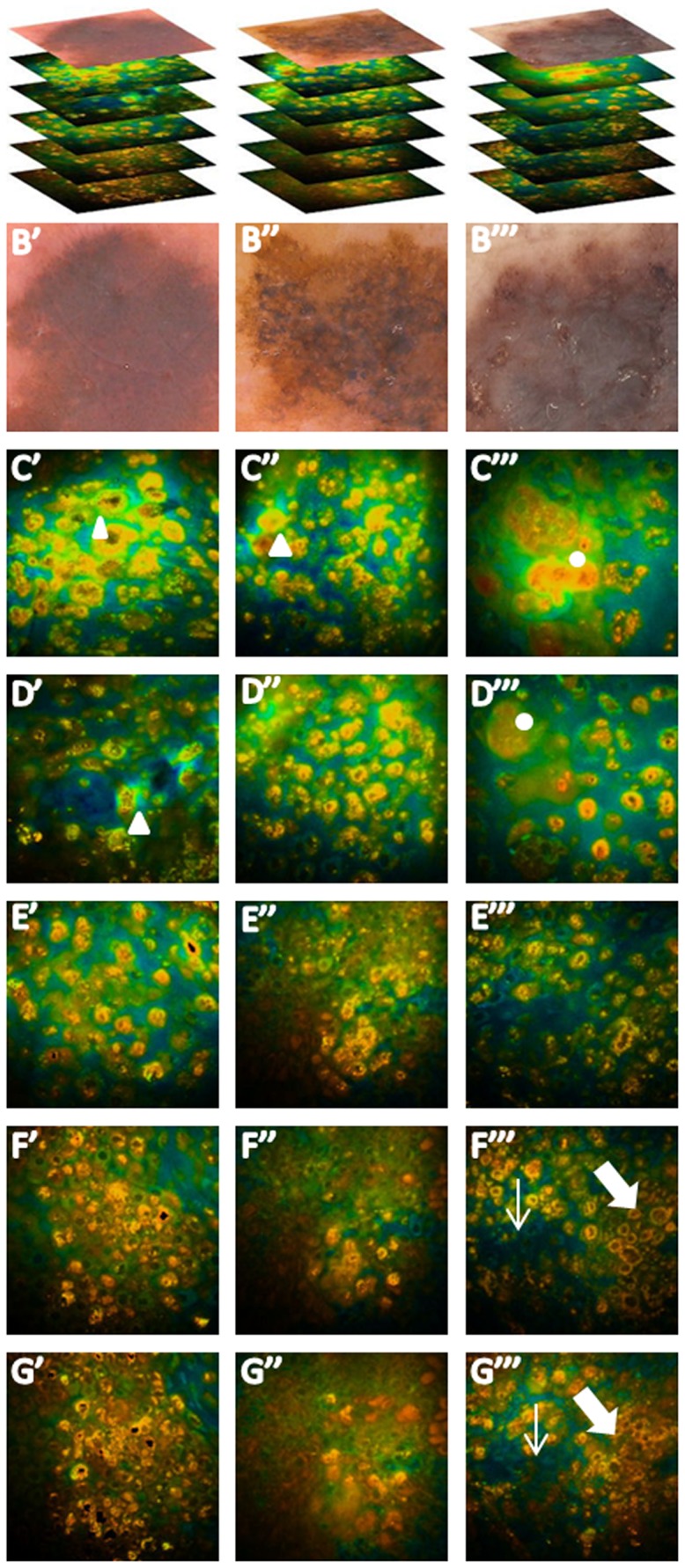
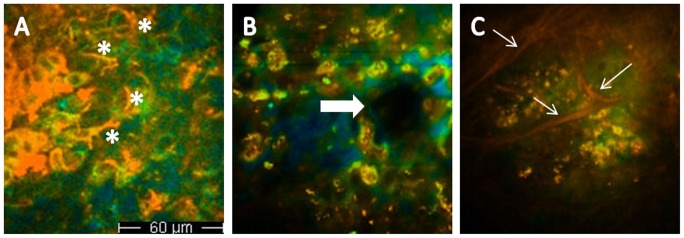
Multiphoton laser tomography (MPT) combined with fluorescence lifetime imaging (FLIM) is a non-invasive imaging technique, based on the study of fluorescence decay times of naturally occurring fluorescent molecules, enabling a non-invasive investigation of the skin with subcellular resolution. The aim of this retrospective observational ex vivo study, was to characterize melanoma both from a morphologic and a quantitative point of view, attaining an improvement in the diagnostic accuracy with respect to dermoscopy. In the training phase, thirty parameters, comprising both cytological descriptors and architectural aspects, were identified. The training set included 6 melanomas with a mean Breslow thickness±S.D. of 0.89±0.48 mm. In the test phase, these parameters were blindly evaluated on a test data set consisting of 25 melanomas, 50 nevi and 50 basal cell carcinomas. Melanomas in the test phase comprised 8 in situ lesions and had a mean thickness±S.D. of 0.77±1.2 mm. Moreover, quantitative FLIM data were calculated for special areas of interest. Melanoma was characterized by the presence of atypical short lifetime cells and architectural disorder, in contrast to nevi presenting typical cells and a regular histoarchitecture. Sensitivity and specificity values for melanoma diagnosis were 100% and 98%, respectively, whereas dermoscopy achieved the same sensitivity, but a lower specificity (82%). Mean fluorescence lifetime values of melanocytic cells did not vary between melanomas and nevi, but significantly differed from those referring to basal cell carcinoma enabling a differential diagnosis based on quantitative data. Data from prospective preoperative trials are needed to confirm if MPT/FLIM could increase diagnostic specificity and thus reduce unnecessary surgical excisions.
Conflict of interest statement
Figures

References
-
- Jemal A, Devesa SS, Hartge P, Tucker MA (2001) Recent trends in cutaneous melanoma incidence among whites in the United States. J Natl Cancer Inst. 93: 678–683. - PubMed
-
- Pellacani G, Lo Scocco G, Vinceti M, Albertini G, Raccagni AA, et al. (2008) Melanoma epidemic across the millennium: time trends of cutaneous melanoma in Emilia-Romagna (Italy) from 1997 to 2004. J Eur Acad Dermatol Venereol 22: 213–218. - PubMed
-
- Bafounta ML, Beauchet A, Aegerter P, Saiag P (2001) Is dermoscopy (epiluminescence microscopy) useful for the diagnosis of melanoma? Results of a meta-analysis using techniques adapted to the evaluation of diagnostic tests. Arch Dermatol 137: 1343–1350. - PubMed
-
- Kittler H, Pehamberger H, Wolff K, Binder M (2002) Diagnostic accuracy of dermoscopy. Lancet Oncol 3: 159–165. - PubMed
-
- Vestergaard ME, Macaskill P, Holt PE, Menzies SW (2008) Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol 159: 669–676. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
