

Neurological features of epilepsy, ataxia, sensorineural deafness, tubulopathy syndrome
- PMID: 23924083
- PMCID: PMC4298033
- DOI: 10.1111/dmcn.12171
Neurological features of epilepsy, ataxia, sensorineural deafness, tubulopathy syndrome
Abstract
Aim: Recently, we reported a previously unrecognized symptom constellation comprising epilepsy, ataxia, sensorineural deafness, and tubulopathy (EAST syndrome) associated with recessive mutations in the KCNJ10 gene. Here, we provide a detailed characterization of the clinical features of the syndrome to aid patient management with respect to diagnosis, prognostic counselling, and identification of best treatment modalities.
Method: We conducted a retrospective review of the detailed neurological and neuroradiological features of nine children (four females, five males; age range at last examination 6-20y) with genetically proven EAST syndrome.
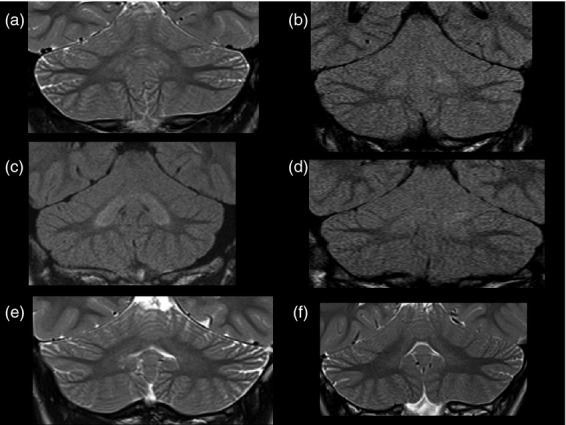
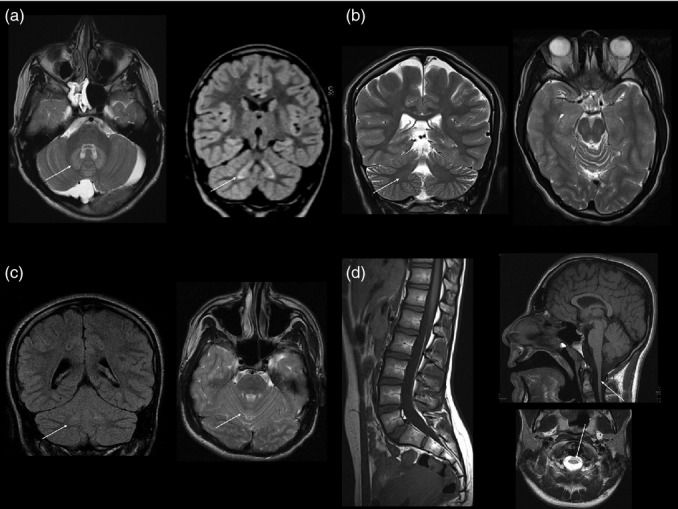
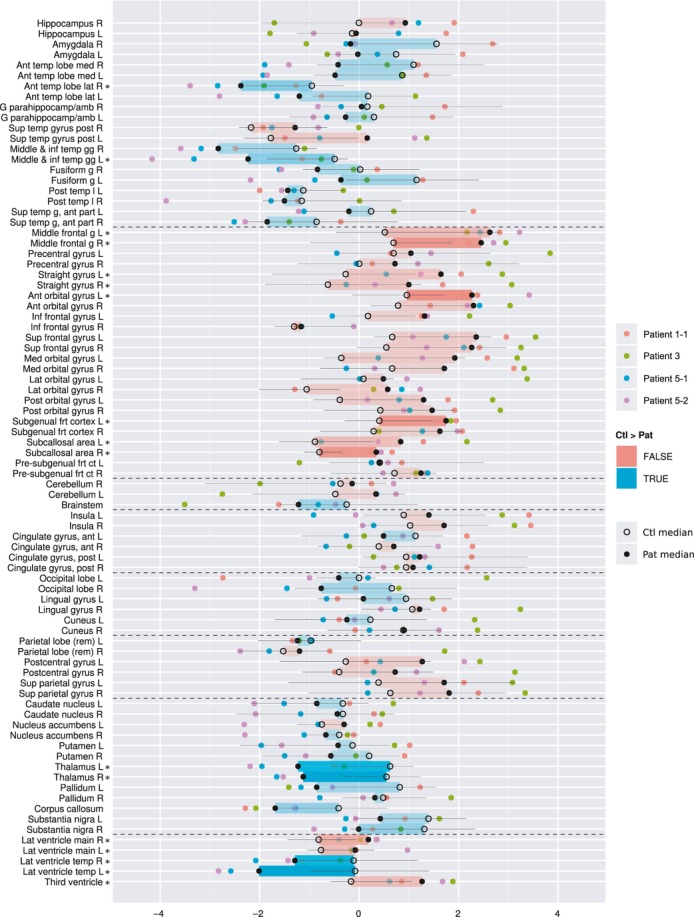
Results: All children presented with tonic-clonic seizures in infancy. Later, non-progressive, cerebellar ataxia and hearing loss were noted. Whilst seizures mostly responded well to treatment, ataxia proved to be the most debilitating feature, with three patients non-ambulant. All available magnetic resonance imaging (MRI) revealed subtle symmetrical signal changes in the cerebellar dentate nuclei. Moreover, four patients had a small corpus callosum and brainstem hypoplasia, and three had a small spinal cord. Regional quantitative volumetric analysis of the images confirmed the corpus callosum and brainstem hypoplasia and showed further patterns of variation from the norm.
Interpretation: The neurological features of EAST syndrome appear to be non-progressive, which is important for prognostic counselling. The spectrum of EAST syndrome includes consistent abnormalities on brain MRI, which may aid diagnosis. Further longitudinal documentation is required to determine the true natural history of the disorder.
© 2013 Mac Keith Press.
Figures
Comment in
-
How the imaging investigation of EAST syndrome points towards the future of radiological multi-parametric phenotyping of a genetic disease.Dev Med Child Neurol. 2013 Sep;55(9):783-4. doi: 10.1111/dmcn.12189. Dev Med Child Neurol. 2013. PMID: 23924081 No abstract available.
References
-
- Bockenhauer D. Ion channels in disease. Curr Opin Pediatr. 2001;13:142–9. - PubMed
-
- Tomlinson SE, Hanna MG, Kullmann DM, Tan SV, Burke D. Clinical neurophysiology of the episodic ataxias: insights into ion channel dysfunction in vivo. Clin Neurophysiol. 2009;120:1768–76. - PubMed
-
- Schwartz PJ, Crotti L. Ion channel diseases in children: manifestations and management. Curr Opin Cardiol. 2008;23:184–91. - PubMed
-
- Lagae L. What's new in: “genetics in childhood epilepsy”. Eur J Pediatr. 2008;167:715–22. - PubMed
-
- Dai AI, Wasay M. Idiopathic epilepsy of childhood and potassium ion channels. J Pak Med Assoc. 2007;57:415–8. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
