

Total laparoscopic pancreaticoduodenectomy
- PMID: 23925010
- PMCID: PMC3771783
- DOI: 10.4293/108680813X13654754534792
Total laparoscopic pancreaticoduodenectomy
Abstract
Introduction: Total laparoscopic pancreaticoduodenectomy (TLPD) remains one of the most advanced laparoscopic procedures. Owing to the evolution in laparoscopic technology and instrumentation within the past decade, laparoscopic pancreaticoduodenectomy is beginning to gain wider acceptance.
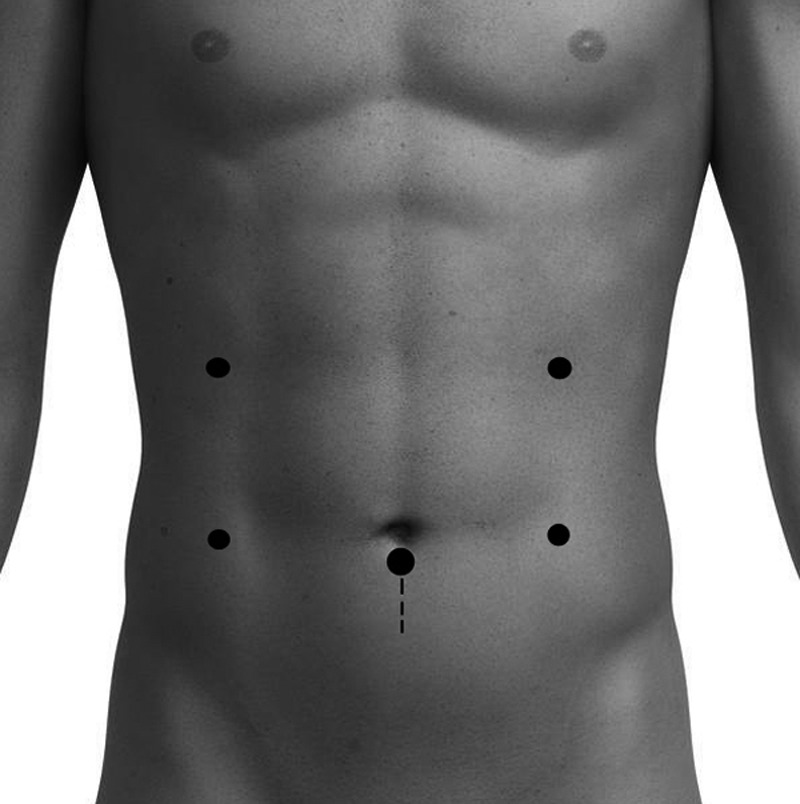
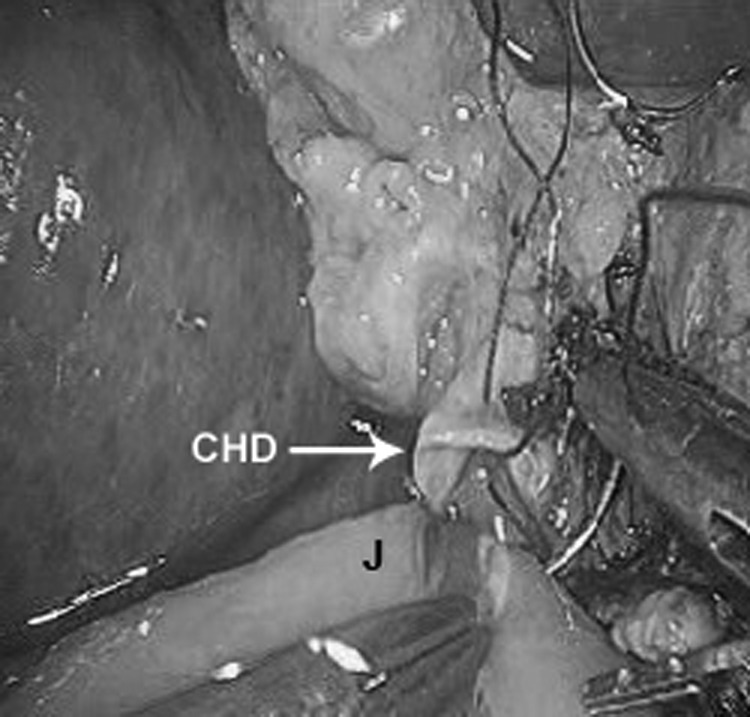
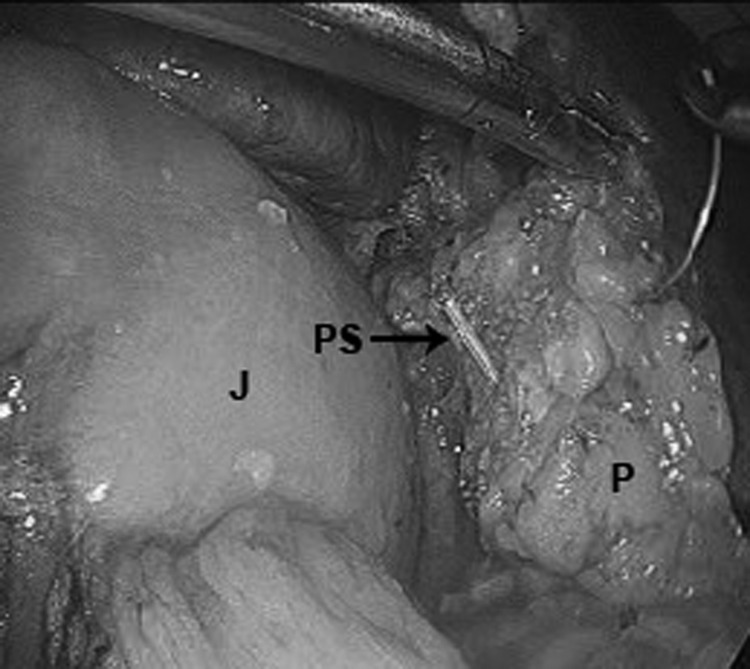
Methods: Data were collected for all patients who underwent a TLPD at our institution. Preoperative evaluation consisted of computed tomography scan with pancreatic protocol and selective use of magnetic resonance imaging and/or endoscopic ultrasonography. The TLPD was done with 6 ports on 3 patients and 5 ports in 2 patients and included a celiac, periportal, peripancreatic, and periduodenal lymphadenectomy. Pancreatic stents were used in all 5 cases, and intestinal continuity was re-established by intracorporeal anastomoses.
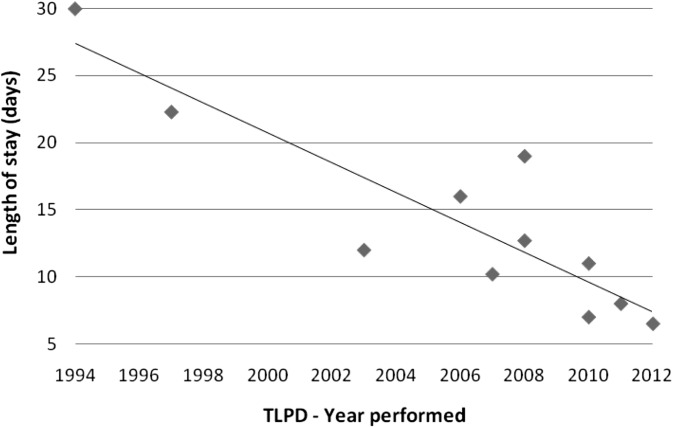
Results: Five patients underwent a TLPD for suspicion of a periampullary tumor. There were 3 women and 2 men with a mean age of 60 years and a mean body mass index of 32.8. Intraoperatively, the mean operative time was 9 hours 48 minutes, with a mean blood loss of 136 mL. Postoperatively, there were no complications and a mean length of stay of 6.6 days. There was no lymph node involvement in 4 out of 5 specimens. The pathological results included intraductal papillary mucinous neoplasm in 2 patients, pancreatic adenocarcinoma in 1 patient (R0 resection), benign 4-cm periampullary adenoma in 1 patient, and a somatostatin neuroendocrine carcinoma in 1 patient (R0, N1).
Conclusion: TLPD is a viable alternative to the standard Whipple procedure. Our early experience suggests decreased length of stay, quicker recovery, and improved quality of life. Complication rates appear to be improved or equivalent.
Figures
References
-
- Gagner M, Palermo M. Laparoscopic Whipple procedure: review of the literature. J Hepatobiliary Pancreat Surg. 2009;16:726–730 - PubMed
-
- Kendrick M, Cusati D. Total laparoscopic pancreaticoduodenectomy. Arch Surg. 2010;145(1):19–23 - PubMed
-
- Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreaticoduodenectomy. Surg Endosc. 1994;8(5):408–410 - PubMed
-
- Gagner M, Pomp A. Laparoscopic pancreatic resection: is it a worthwhile? J Gastrointest Surg. 1997;1(1):20–25, discussion 25–26 - PubMed
-
- Masson B, Sa-Cunha A, Laurent C, et al. Laparoscopic pancreatectomy: report of 22 cases. Ann Chir. 2003;128(7):452–456 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous