

Malignant hyperthermia during laparoscopic adjustable gastric banding
- PMID: 23925035
- PMCID: PMC3771808
- DOI: 10.4293/108680813X13693422521278
Malignant hyperthermia during laparoscopic adjustable gastric banding
Abstract
Background: We report a rare case of malignant hyperthermia during laparoscopic adjustable gastric banding.
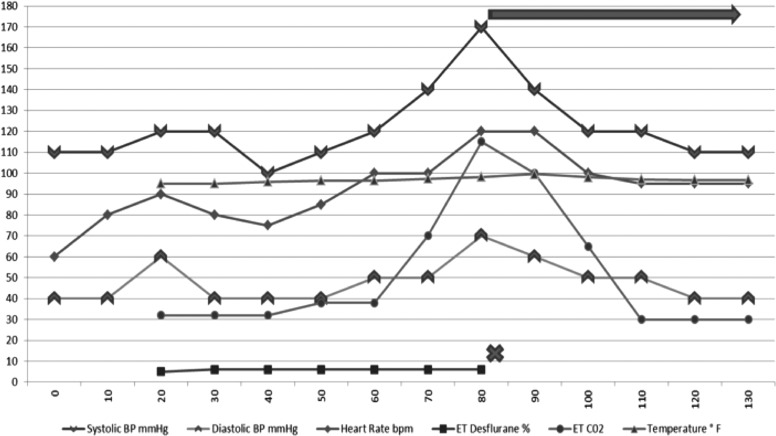
Case description: A 32-y-old female with no previous history of adverse reaction to general anesthesia underwent laparoscopic adjustable gastric banding. Intraoperative monitoring revealed a sharp increase in end-tidal carbon dioxide, autonomic instability, and metabolic and respiratory acidosis, along with other metabolic and biochemical derangements. She was diagnosed with malignant hyperthermia. Desflurane, the anesthetic agent was discontinued, and the patient was started on intravenous dantrolene.
Results: The surgery was completed, and the patient was brought to the surgical intensive care unit for continued postoperative care. She developed muscle weakness and phlebitis that resolved prior to discharge.
Conclusion: Prompt diagnosis and treatment of malignant hyperthermia leads to favorable clinical outcome. This clinical entity can occur in the bariatric population with the widely used desflurane. Bariatric surgeons and anesthesiologists alike must be aware of the early clinical signs of this rare, yet potentially fatal, complication.
Figures
References
-
- Chapman AE, Kiroff G, Game P, et al. Laparoscopic adjustable gastric banding in the treatment of obesity: a systematic literature review. Surgery. 2004;135(3):326–351 - PubMed
-
- Parikh MS, Shen R, Weiner M, Siegel N, Ren CJ. Laparoscopic bariatric surgery in super-obese patients (BMI>50) is safe and effective: a review of 332 patients. Obes Surg. 2005;15(6):858–863 - PubMed
-
- O'Brien PE, Dixon JB. Lap-band: outcomes and results. J Laparoendosc Adv Surg Tech A. 2003;13(4):265–270 - PubMed
-
- Carelli AM, Youn HA, Kurian MS, Ren CJ, Fielding GA. Safety of the laparoscopic adjusted gastric band: 7-year data from a U.S. center of excellence. Surg Endosc. 2010;24(8):1819–1823 - PubMed
-
- Ren CJ, Horgan S, Ponce J. US experience with the LAP-BAND system. Am J Surg. 2002;184(6B):46S–50S - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources