

Imaging modalities in keratoconus
- PMID: 23925322
- PMCID: PMC3775072
- DOI: 10.4103/0301-4738.116058
Imaging modalities in keratoconus
Abstract
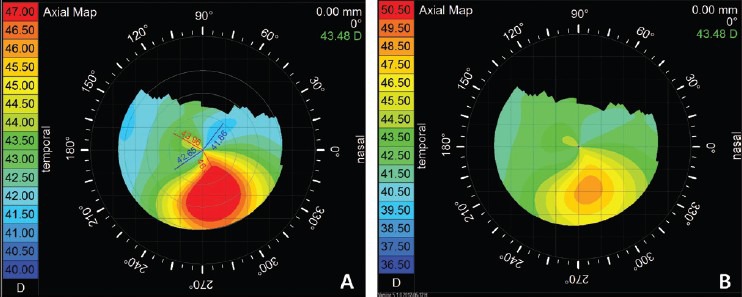
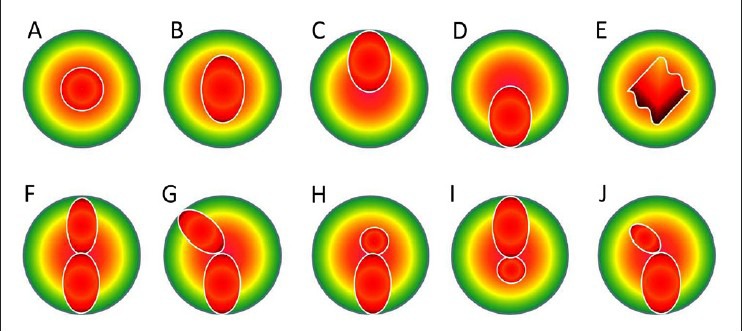
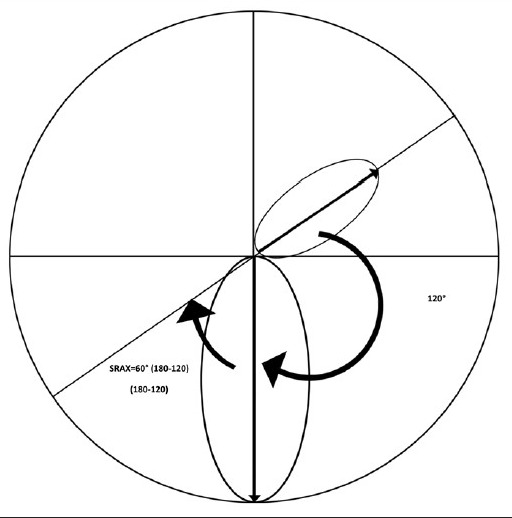
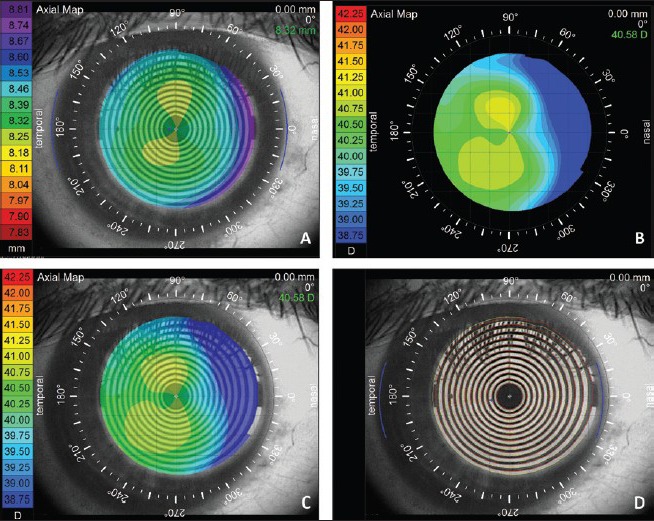
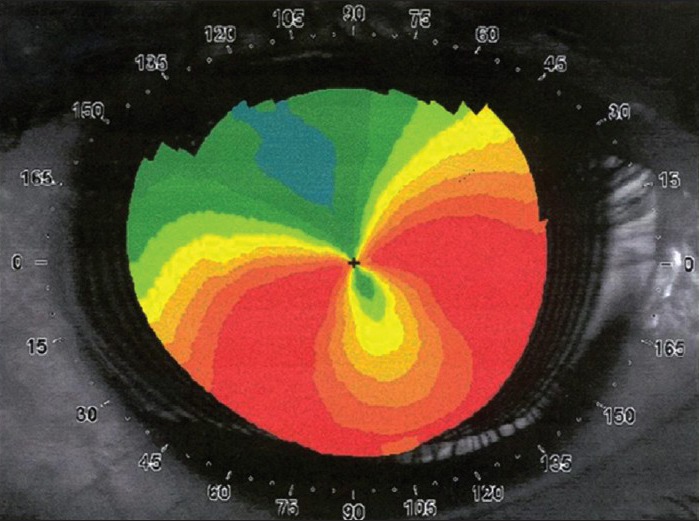
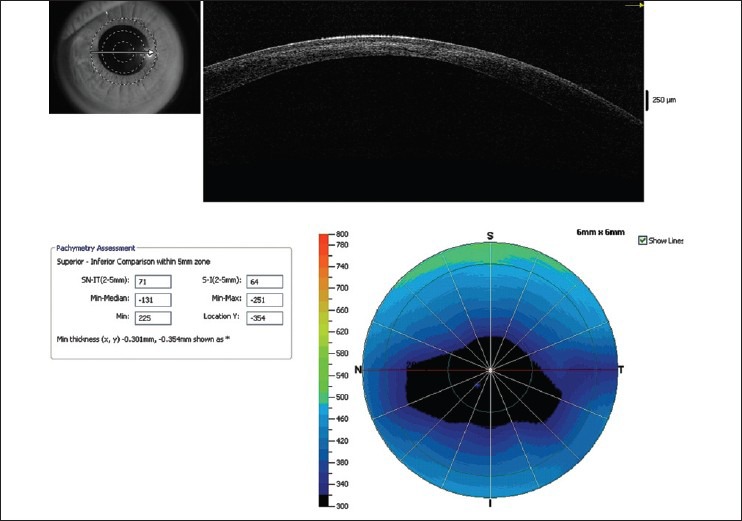
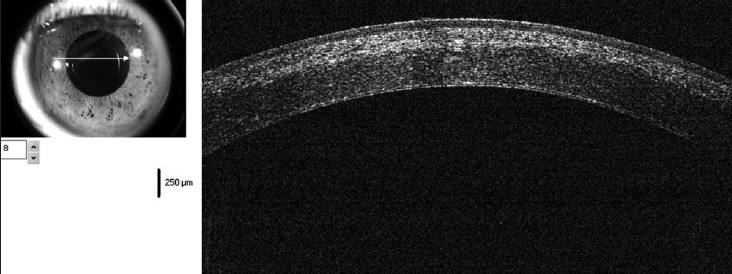
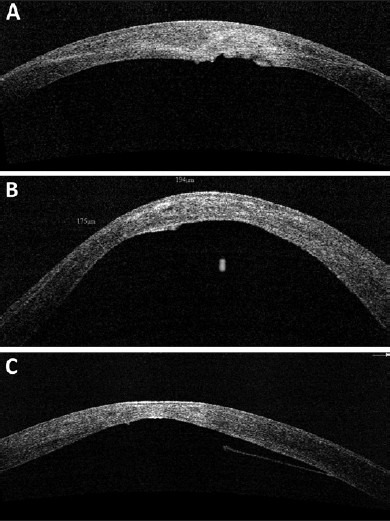
Diagnosis of keratoconus has greatly improved from simple clinical diagnosis with the advent of better diagnostic devices like corneal topographers based on placido disc, elevation based topographers and lately optical coherence tomography (OCT). These instruments are quite sensitive to pick up early keratoconus, which could help refractive surgeons to avoid serious complications like ectasia following keratorefractive surgeries. Each of these instruments has their advantages and disadvantages; in spite of that each one of them has its own place in the clinical practice. Currently, placido disc based topographers are the most commonly used topographers all over the world. There are many different companies making such devices, which follow the different techniques and color for the display. Due to these differences they are not directly comparable to each other. Various quantitative indices based on these topographers have been suggested and validated by different authors to aid in the diagnosis and quantification of keratoconus. OCT with its higher resolution and deeper penetration has created its place in the diagnostic armamentarium for keratoconus.
Conflict of interest statement
Figures
References
-
- Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322. - PubMed
-
- Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. - PubMed
-
- Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110:267–75. - PubMed
-
- Mazzotta C, Balestrazzi A, Traversi C, Baiocchi S, Caporossi T, Tommasi C, et al. Treatment of progressive keratoconus by riboflavin-UVA-induced cross-linking of corneal collagen: Ultrastructural analysis by Heidelberg Retinal Tomograph II in vivo confocal microscopy in humans. Cornea. 2007;26:390–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
