

Morphea in adults and children cohort III: nested case-control study--the clinical significance of autoantibodies in morphea
- PMID: 23925398
- PMCID: PMC4153681
- DOI: 10.1001/jamadermatol.2013.4207
Morphea in adults and children cohort III: nested case-control study--the clinical significance of autoantibodies in morphea
Abstract
Importance: Small studies have implicated the association of specific autoantibodies with morphea subtype or severity, but no large-scale studies have been conducted. This prospective case-control study confirmed the presence of antinuclear antibodies (ANAs) and other autoantibodies in morphea but found they are of limited significance.
Objective: To determine the prevalence of ANAs, extractable nuclear antigens such as antihistone antibodies (AHAs), and anti-single-stranded DNA antibodies (ssDNA abs) in patients with morphea vs a healthy control population and their association with clinical measures of morphea severity.
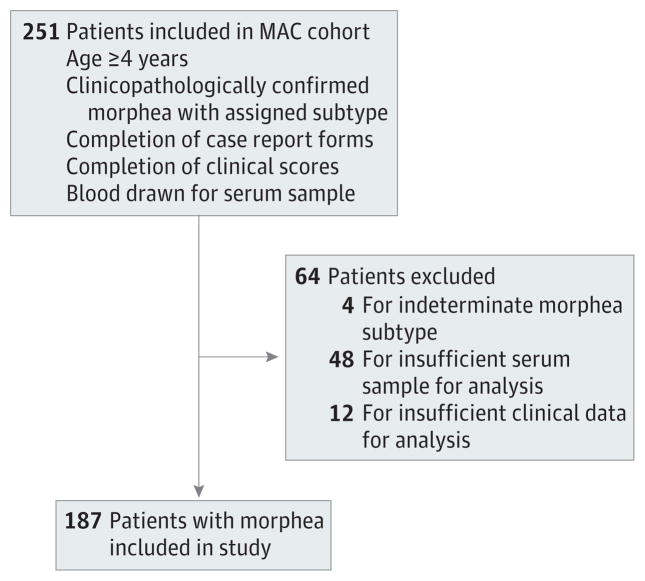
Design, setting, and participants: Nested case-control study, conducted at the University of Texas Southwestern Medical Center, Dallas, and University of Texas Health Science Center, Houston. Study participants included individuals enrolled in the Morphea in Adults and Children (MAC) cohort and Scleroderma Family Registry and DNA Repository.
Main outcomes and measures: Prevalence of ANAs, AHAs, ssDNA abs in patients with morphea vs matched controls and association of the presence of autoantibodies with clinical indicators of morphea severity.
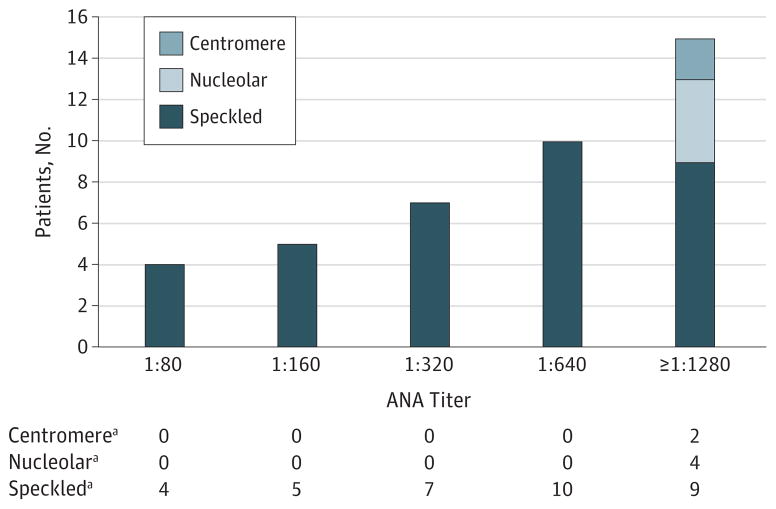
Results: The prevalence of ANAs, AHAs, and ssDNA abs in patients with morphea was 34%, 12%, and 8%, respectively. Antinuclear antibodies and AHAs, but not ssDNA abs, were present more frequently in cases than in controls. There was no difference in ANA prevalence among morphea subtypes. Among patients with linear morphea, the presence of autoantibodies was associated with clinical indicators of severe morphea including functional limitation (ssDNA ab, P = .005; and AHA, P = .006), extensive body surface area involvement (ssDNA ab, P = .01; and ANA, P = .005), and higher skin scores (ANA, P = .004). The presence of autoantibodies was not associated with clinical measures of morphea activity.
Conclusions and relevance: Our results demonstrate that ANAs and AHAs are more prevalent among patients with morphea but are of limited clinical utility except in linear morphea, where their presence, although infrequent, is associated with greater lesion burden and functional impairment.
Conflict of interest statement
Figures
Comment in
-
Practice gaps: Evaluating the clinical utility of autoantibodies in morphea.JAMA Dermatol. 2013 Oct;149(10):1166. doi: 10.1001/jamadermatol.2013.4908. JAMA Dermatol. 2013. PMID: 23925297 No abstract available.
References
-
- Zulian F, Athreya BH, Laxer R, et al. Juvenile Scleroderma Working Group of the Pediatric Rheumatology European Society (PRES) Juvenile localized scleroderma: clinical and epidemiological features in 750 children: an international study. Rheumatology (Oxford) 2006;45(5):614–620. - PubMed
-
- Martini G, Murray KJ, Howell KJ, et al. Juvenile-onset localized scleroderma activity detection by infrared thermography. Rheumatology (Oxford) 2002;41(10):1178–1182. - PubMed
-
- Li SC, Liebling MS, Haines KA. Ultrasonography is a sensitive tool for monitoring localized scleroderma. Rheumatology (Oxford) 2007;46(8):1316–1319. - PubMed
-
- Arkachaisri T, Fertig N, Pino S, Medsger TA., Jr Serum autoantibodies and their clinical associations in patients with childhood- and adult-onset linear scleroderma: a single-center study. J Rheumatol. 2008;35(12):2439–2444. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
