

Framework for understanding balance dysfunction in Parkinson's disease
- PMID: 23925954
- PMCID: PMC4001822
- DOI: 10.1002/mds.25613
Framework for understanding balance dysfunction in Parkinson's disease
Abstract
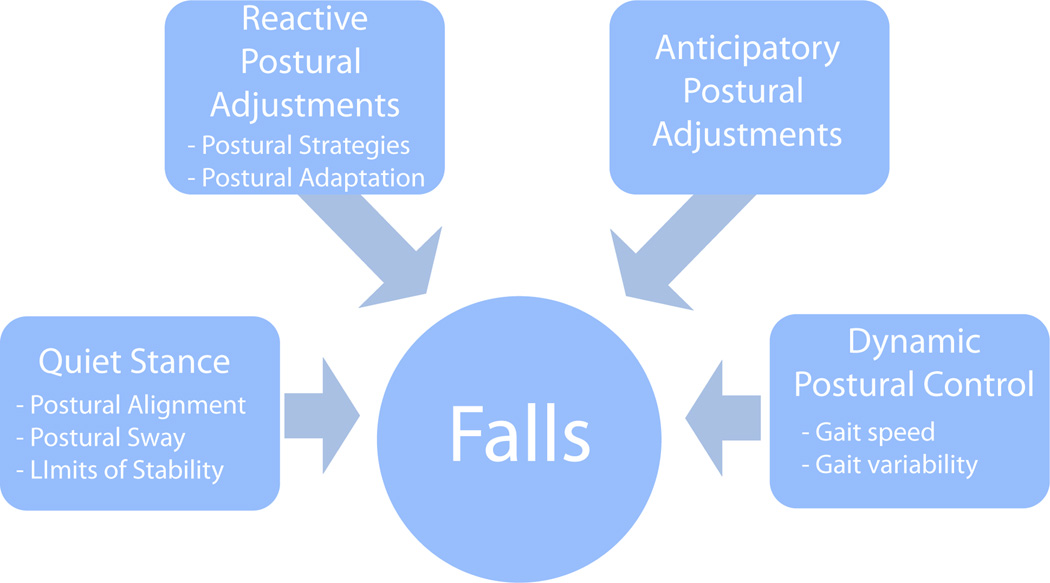
People with Parkinson's disease (PD) suffer from progressive impairment in their mobility. Locomotor and balance dysfunction that impairs mobility in PD is an important cause of physical and psychosocial disability. The recognition and evaluation of balance dysfunction by the clinician are an essential component of managing PD. In this review, we describe a framework for understanding balance dysfunction in PD to help clinicians recognize patients who are at risk for falling and impaired mobility.
Keywords: Parkinson's disease; balance; gait; posture.
© 2013 Movement Disorder Society.
Conflict of interest statement
Fay Horak and OHSU have significant financial interests in APDM, a company that might have a commercial interest in the results of this research and technology. This potential conflict of interest has been reviewed and managed by OHSU and the Integrity Oversight Council.
John Nutt serves as a consultant for Neuroderm Ltd, Merck, Elan Pharmaceuticals, Lundbeck Inc, ONO Pharma, SynAgile Crop, Prexa Inc and US World Med. He has received honoraria from the American Academy of Neurology.
Figures
References
-
- Bloem BR, Hausdorff JM, Visser JE, et al. Falls and freezing of gait in Parkinson's disease: a review of two interconnected, episodic phenomena. Mov Disord. 2004;19:871–884. - PubMed
-
- Horak FB, Macpherson JM. Handbook of Physiology. New York: Oxford University Press; 1996. Postural orientation and equilibrium: Interaction and coordination; pp. 255–292.
-
- Burleigh A, Horak F, Nutt J, et al. Levodopa reduces muscle tone and lower extremity tremor in Parkinson's disease. Can J Neurol Sci. 1995;22:280–285. - PubMed
-
- Bloem BR, Beckley DJ, van Dijk JG. Are automatic postural responses in patients with Parkinson's disease abnormal due to their stooped posture? Exp Brain Res. 1999;124:481–488. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
