

Is a Plasmodium lactate dehydrogenase (pLDH) enzyme-linked immunosorbent (ELISA)-based assay a valid tool for detecting risky malaria blood donations in Africa?
- PMID: 23927596
- PMCID: PMC3750723
- DOI: 10.1186/1475-2875-12-279
Is a Plasmodium lactate dehydrogenase (pLDH) enzyme-linked immunosorbent (ELISA)-based assay a valid tool for detecting risky malaria blood donations in Africa?
Abstract
Background: Malaria is a leading cause of mortality in southern Benin. The main causative agent, Plasmodium falciparum, poses a threat on critical transfusions in pregnant women and children. This study's objective was to compare the performance of different malaria screening methods in blood donors in southern Benin, a malaria-endemic country.
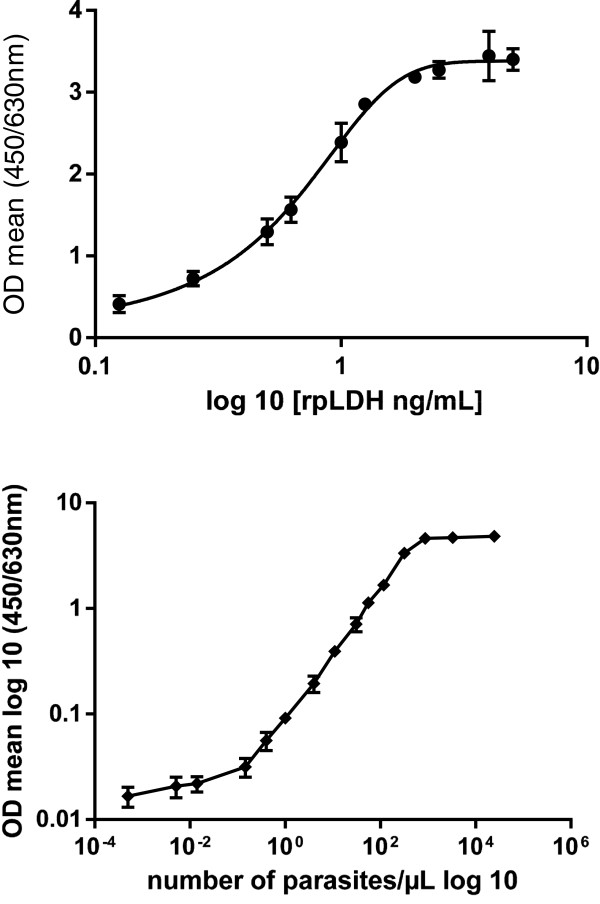
Methods: Blood from 2,515 voluntary blood donors in Benin was collected over a period of 10 months in ethylenediaminetetraacetic acid (EDTA) tubes, which were then classified according to extraction time: long rainy season, short dry season, short rainy season, and long dry season. Microscopic examination was used to count parasites. Parasite density (PD) was expressed as the number of parasites per μL of blood. Pan Plasmodium pLDH detection was assessed by an ELISA-malaria antigen test. Using crude soluble P. falciparum antigens, an ELISA-malaria antibody test detected anti-Plasmodium antibodies.
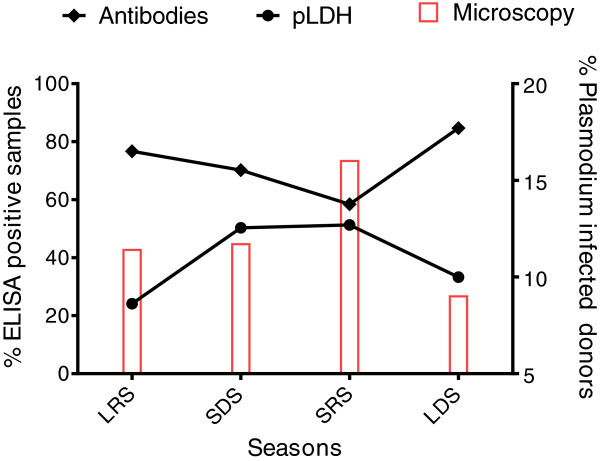
Results: Among the 2,515 blood donors (2,025 males and 488 females) screened, the rate of asymptomatic Plasmodium carriage was 295/2,515 (11.72%, 95% CI: 10.5-13.1%). Males had a higher infection rate (12.4%) than did females (8.8%). Parasite density was very low: between seven and100 parasites per μL of blood was reported in 80% of donors with parasitaemia. Three Plasmodium species were diagnosed: P. falciparum in 280/295 patients (95.0%), Plasmodium malariae in 14/295 (5.0%), and Plasmodium ovale in 1/295 (0.34%). Malaria prevalence in donors was higher during the rainy seasons (13.7%) compared with the dry seasons (9.9%). The use of a highly sensitive assay enabled pan Plasmodium pLDH detection in 966/2,515 (38.4%, 95% CI: 36.5%-40.3%). Malaria antibody prevalence was 1,859/2,515 (73.9%, 95% CI: 72.16-75.6%). Donors' antigenaemia and antibody levels varied significantly (P <0.05) over the course of the four seasons. The highest antigenaemia rate 323/630 (51.3%), was observed during the short rainy season, while the highest antibody prevalence, 751/886 (84.7%), was recorded during the long dry season.
Conclusion: Blood donations infected with Plasmodium can transmit malaria to donation recipients. Malaria diagnostic methods are currently available, but the feasibility criteria for mass screening in endemic areas become preponderant. Detection of the pLDH antigen seems to be an adequate screening tool in endemic areas, for this antigen indicates parasite presence. Routine screening of all donated blood would prevent infected blood donations and reduce P. falciparum transmission in critical patients, such as children and pregnant women. This tool would also decrease medical prophylaxis in donation recipients and contribute to lower Plasmodium resistance.
Figures
Similar articles
-
Comparative evaluation of a rapid diagnostic test, an antibody ELISA, and a pLDH ELISA in detecting asymptomatic malaria parasitaemia in blood donors in Buea, Cameroon.Infect Dis Poverty. 2017 Aug 1;6(1):103. doi: 10.1186/s40249-017-0314-2. Infect Dis Poverty. 2017. PMID: 28760158 Free PMC article.
-
Comparison of PfHRP-2/pLDH ELISA, qPCR and microscopy for the detection of plasmodium events and prediction of sick visits during a malaria vaccine study.PLoS One. 2013;8(3):e56828. doi: 10.1371/journal.pone.0056828. Epub 2013 Mar 15. PLoS One. 2013. PMID: 23554856 Free PMC article. Clinical Trial.
-
[Prevention of transfusion transmitted malaria in endemic area].Transfus Clin Biol. 2009 Nov-Dec;16(5-6):454-9. doi: 10.1016/j.tracli.2009.02.004. Epub 2009 Aug 7. Transfus Clin Biol. 2009. PMID: 19665412 French.
-
Laboratory detection of donors implicated in transfusion-transmitted malaria.Transfusion. 2024 Dec;64(12):2325-2331. doi: 10.1111/trf.18061. Epub 2024 Nov 6. Transfusion. 2024. PMID: 39503566 Free PMC article. Review.
-
Exploring Biomarkers for Malaria: Advances in Early Detection and Asymptomatic Diagnosis.Biosensors (Basel). 2025 Feb 12;15(2):106. doi: 10.3390/bios15020106. Biosensors (Basel). 2025. PMID: 39997008 Free PMC article. Review.
Cited by
-
DNA Sequence Polymorphism of the Lactate Dehydrogenase Genefrom Iranian Plasmodium vivax and Plasmodium falciparum Isolates.Iran J Parasitol. 2015 Oct-Dec;10(4):505-16. Iran J Parasitol. 2015. PMID: 26811715 Free PMC article.
-
The ears of the African elephant: unexpected high seroprevalence of Plasmodium ovale and Plasmodium malariae in healthy populations in Western Africa.Malar J. 2014 Jun 18;13:240. doi: 10.1186/1475-2875-13-240. Malar J. 2014. PMID: 24946685 Free PMC article.
-
Comparative evaluation of the diagnostic accuracies of four different malaria rapid diagnostic test kits available in Ghana.PLoS One. 2024 May 7;19(5):e0302840. doi: 10.1371/journal.pone.0302840. eCollection 2024. PLoS One. 2024. PMID: 38713676 Free PMC article.
-
The hide and seek of Plasmodium vivax in West Africa: report from a large-scale study in Beninese asymptomatic subjects.Malar J. 2016 Nov 25;15(1):570. doi: 10.1186/s12936-016-1620-z. Malar J. 2016. PMID: 27887647 Free PMC article.
-
Dielectrophoresis for Biomedical Sciences Applications: A Review.Sensors (Basel). 2017 Feb 24;17(3):449. doi: 10.3390/s17030449. Sensors (Basel). 2017. PMID: 28245552 Free PMC article. Review.
References
-
- Woolsey. Transfusion for pernicious anaemia: two cases. Ann Surg. 1991;53:132–135.
-
- Wylie BR. Transfusion transmitted infection: viral and exotic diseases. Anaesth Intensive Care. 1993;21:24–30. - PubMed
-
- Kinde G, Oke J, Gnahoui I, Massougbodji A. [The risk of malaria transmission by blood transfusion at Cotonou, Benin](in French) Sante. 2000;10:389–392. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
