

Automatic magnetic resonance spinal cord segmentation with topology constraints for variable fields of view
- PMID: 23927903
- PMCID: PMC3823375
- DOI: 10.1016/j.neuroimage.2013.07.060
Automatic magnetic resonance spinal cord segmentation with topology constraints for variable fields of view
Abstract
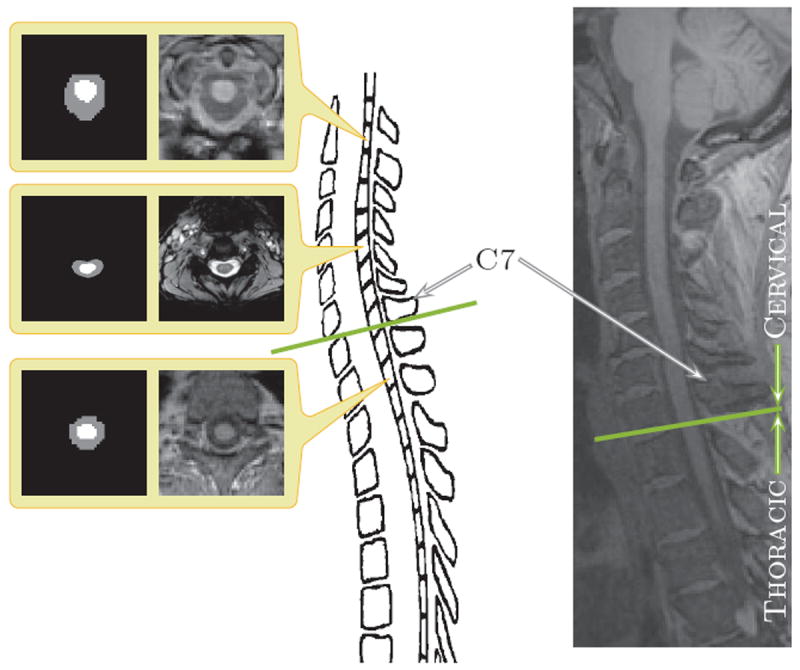
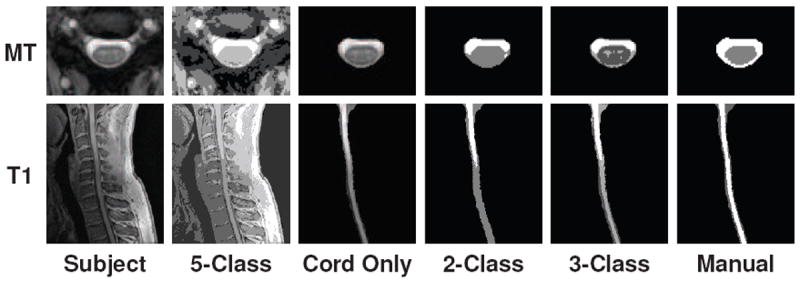
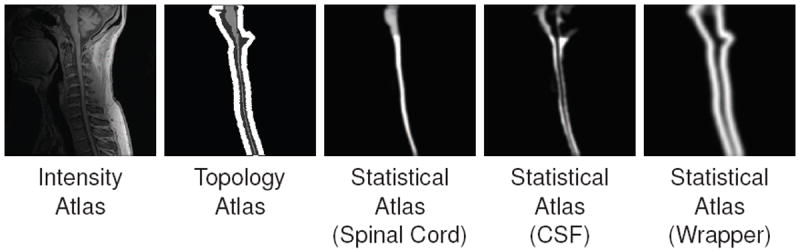
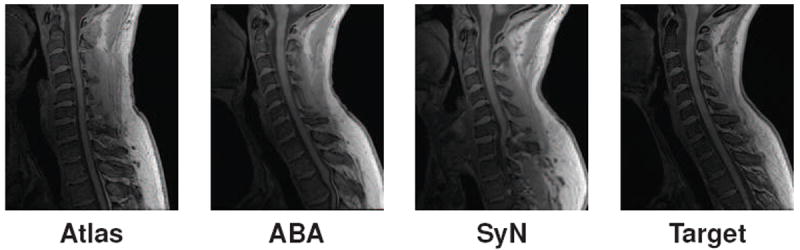
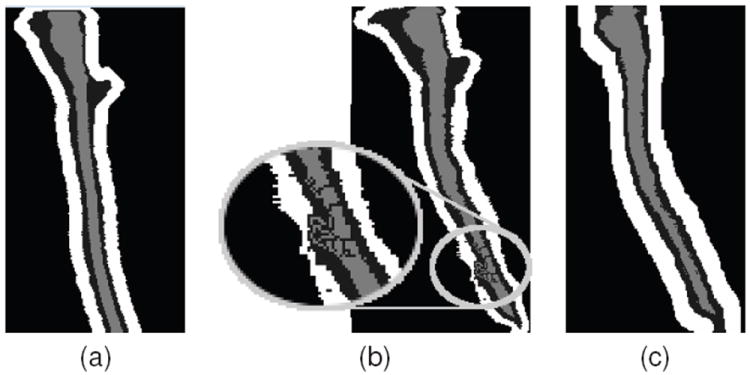
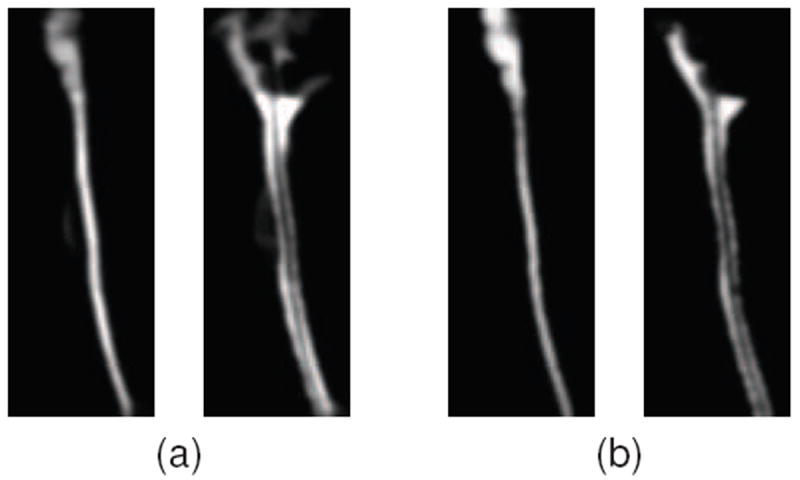
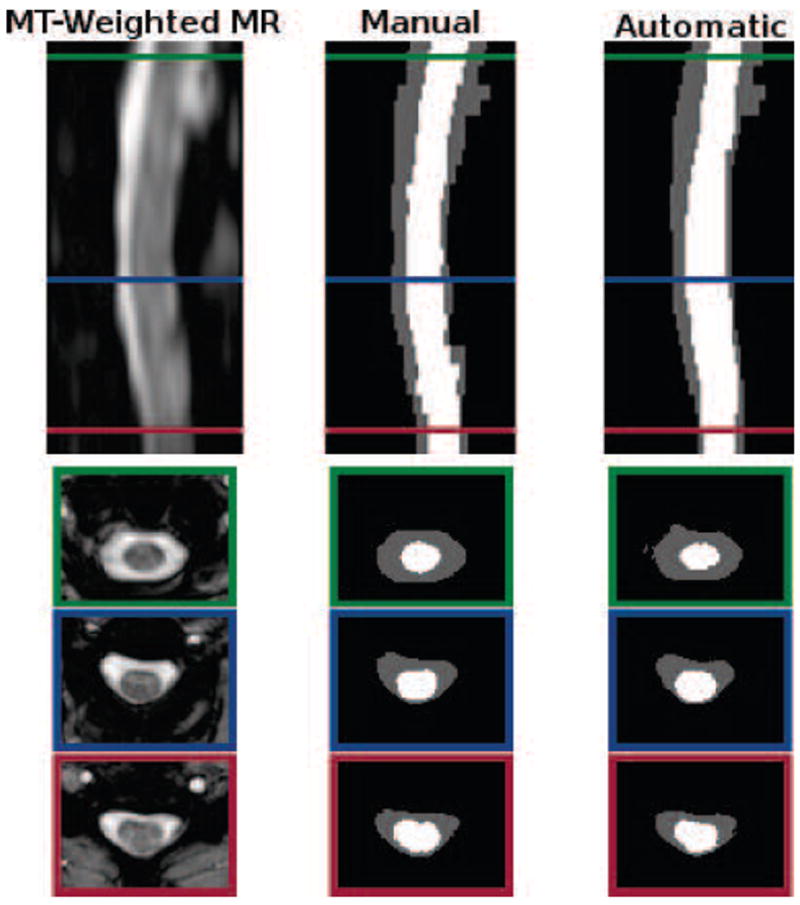
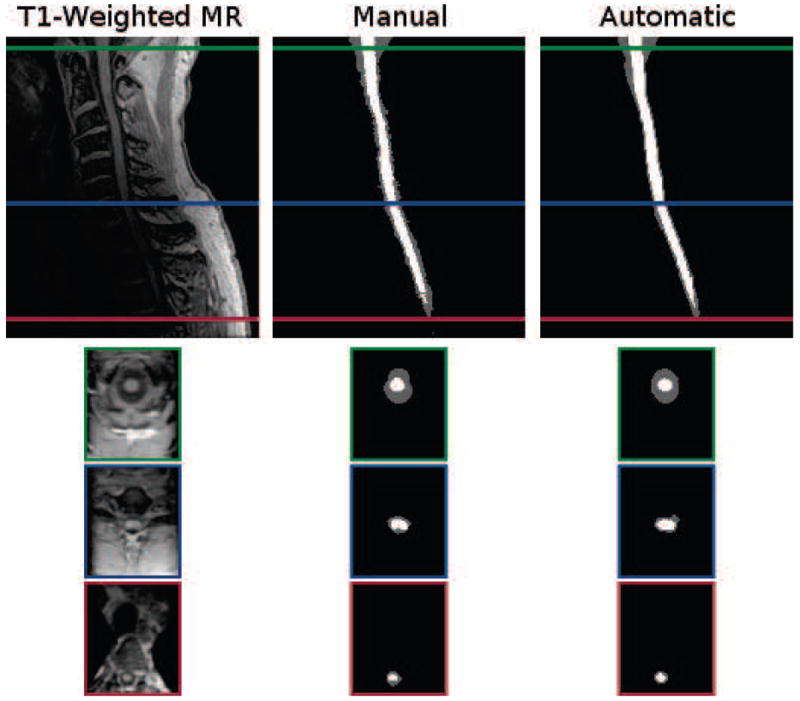
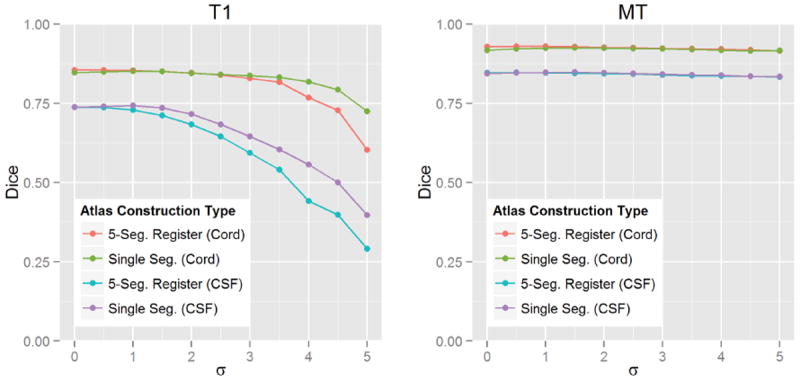
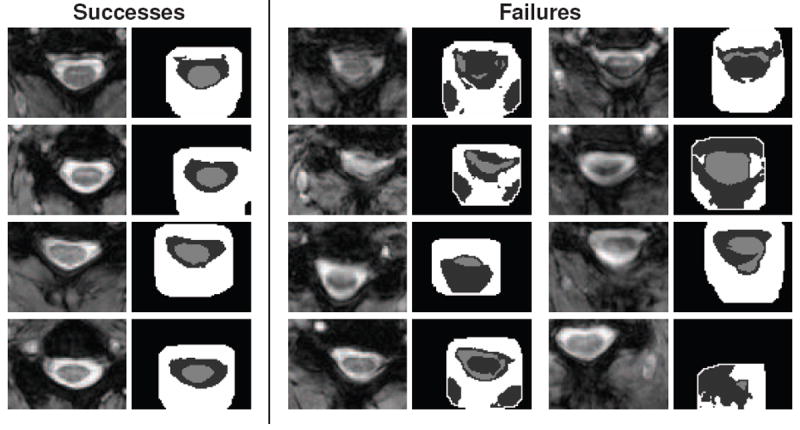
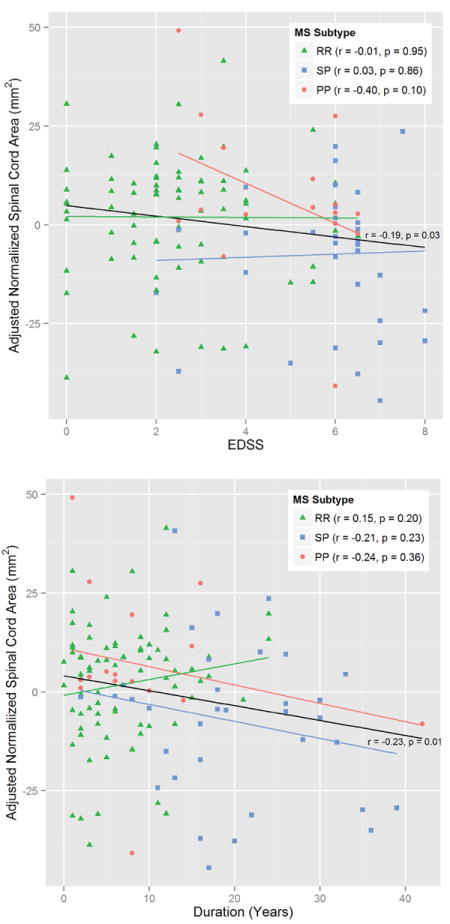
Spinal cord segmentation is an important step in the analysis of neurological diseases such as multiple sclerosis. Several studies have shown correlations between disease progression and metrics relating to spinal cord atrophy and shape changes. Current practices primarily involve segmenting the spinal cord manually or semi-automatically, which can be inconsistent and time-consuming for large datasets. An automatic method that segments the spinal cord and cerebrospinal fluid from magnetic resonance images is presented. The method uses a deformable atlas and topology constraints to produce results that are robust to noise and artifacts. The method is designed to be easily extended to new data with different modalities, resolutions, and fields of view. Validation was performed on two distinct datasets. The first consists of magnetization transfer-prepared T2*-weighted gradient-echo MRI centered only on the cervical vertebrae (C1-C5). The second consists of T1-weighted MRI that covers both the cervical and portions of the thoracic vertebrae (C1-T4). Results were found to be highly accurate in comparison to manual segmentations. A pilot study was carried out to demonstrate the potential utility of this new method for research and clinical studies of multiple sclerosis.
Keywords: Atlas construction; Digital homeomorphism; Magnetic resonance imaging; Spinal cord segmentation; Topology-preserving segmentation.
© 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Archip N, Erard PJ, Egmont-Petersen M, Haefliger JM, Germond JF. A Knowledge-Based Approach to Automatic Detection of the Spinal Cord in CT Images. IEEE Trans Med Imag. 2002;21(12):1504–1516. - PubMed
-
- Bazin PL, Ellingsen LM, Pham DL. Digital homeomorphisms in deformable registration. Proceedings of the International Conference on Information Processing in Medical Imaging (IPMI ’07); 2007. pp. 211–222. - PubMed
-
- Bezdek JC. A Convergence Theorem for the Fuzzy ISODATA Clustering Algorithms. IEEE Trans on Pattern Anal Machine Intell. 1980;2(1):1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
