

Renal physiology of pregnancy
- PMID: 23928384
- PMCID: PMC4089195
- DOI: 10.1053/j.ackd.2013.01.012
Renal physiology of pregnancy
Abstract
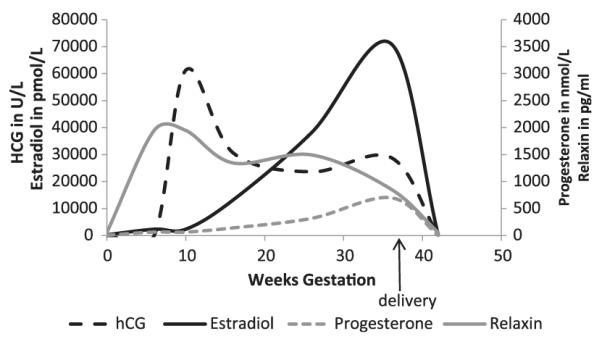
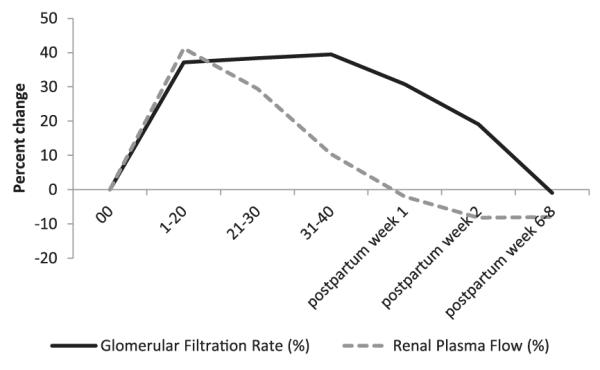
Pregnancy involves remarkable orchestration of physiologic changes. The kidneys are central players in the evolving hormonal milieu of pregnancy, responding and contributing to the changes in the environment for the pregnant woman and fetus. The functional impact of pregnancy on kidney physiology is widespread, involving practically all aspects of kidney function. The glomerular filtration rate increases 50% with subsequent decrease in serum creatinine, urea, and uric acid values. The threshold for thirst and antidiuretic hormone secretion are depressed, resulting in lower osmolality and serum sodium levels. Blood pressure drops approximately 10 mmHg by the second trimester despite a gain in intravascular volume of 30% to 50%. The drop in systemic vascular resistance is multifactorial, attributed in part to insensitivity to vasoactive hormones, and leads to activation of the renin-aldosterone-angiostensin system. A rise in serum aldosterone results in a net gain of approximately 1000 mg of sodium. A parallel rise in progesterone protects the pregnant woman from hypokalemia. The kidneys increase in length and volume, and physiologic hydronephrosis occurs in up to 80% of women. This review will provide an understanding of these important changes in kidney physiology during pregnancy, which is fundamental in caring for the pregnant patient.
Copyright © 2013 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Dunlop W. Serial changes in renal hemodynamics during normal human pregnancy. Br J Obstet Gynaecol. 1981;88(1):1–9. - PubMed
-
- Harrow BR, Sioan JA, Salhanick L. Etiology of the hydronephrosis of pregnancy. Surg Gynecol Obstet. 1964;119:1042–1048. - PubMed
-
- Rasmussen PE, Nielson FR. Hydronephrosis in pregnancy: a literature survey. Eur J Obstet Gynecol Reprod Biol. 1988;27(3):249–259. - PubMed
-
- Faundes A, Bricola-Filho M, Pinto e Silva JL. Dilatation of the urinary tract during pregnancy: proposal of a curve of maximal caliceal diameter by gestational age. Am J Obstet Gynecol. 1998;178(5):1082–1086. - PubMed
-
- Cietak KA, Newton JR. Serial quantitative maternal nephrosonography in pregnancy. Br J Radiol. 1985;58(689):405–413. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
