

Review
doi: 10.1053/j.ackd.2013.01.014.
The management of hypertension in pregnancy
Affiliations
- PMID: 23928387
- PMCID: PMC3925675
- DOI: 10.1053/j.ackd.2013.01.014
Item in Clipboard
Review
The management of hypertension in pregnancy
Adv Chronic Kidney Dis.
2013 May.
Abstract
Hypertensive pregnancy disorders complicate 6% to 8% of pregnancies and cause significant maternal and fetal morbidity and mortality. The goal of treatment is to prevent significant cerebrovascular and cardiovascular events in the mother without compromising fetal well-being. Current guidelines differentiate between the treatment of women with acute hypertensive syndromes of pregnancy and women with preexisting chronic hypertension in pregnancy. This review will address the management of hypertension in pregnancy, review the various pharmacologic therapies, and discuss the future directions in this field.
Copyright © 2013 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
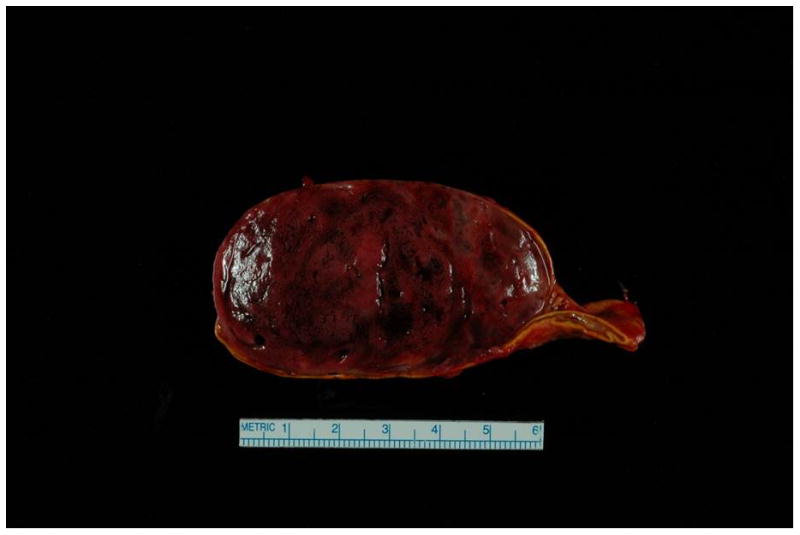
Surgical specimen of the adrenal pheochromocytoma. Case presentation - Patient was a 31 year old P6G5 with a history of chronic hypertension requiring medications intermittently in the past, and a history of preeclampsia with her first pregnancy, with subsequent unremarkable pregnancies. She was admitted at 34 weeks due to systolic BP > 200 mm Hg, as well as 3+ protein on dipstick, elevated AST (57 U/L), serum creatinine of 1.2 mg/dL and uric acid of 10.1 mg/dL. The constellation of clinical findings and laboratory abnormalities was considered to be consistent with preeclampsia. She received IV magnesium sulfate and labetalol, and underwent C-section at 34 and 4/7 weeks, and gave birth to a healthy male infant. Systolic BPs remained in the 180s mm Hg post-delivery, and she was transferred to the ICU for hypertensive urgency. Work-up for secondary causes revealed a 3.2 × 6.2 × 5.3 cm heterogenous lesion in the right adrenal gland, and MRI was consistent with pheochromocytoma. The level of plasma free normetanephrine was 26.2 nmol/L (normal < 0.90 nmol/L), and the 24-hour urine showed significantly elevated levels of norepinephrine and normetanephrine. She received phenoxybenzamine, nicardipine and propranolol. She underwent a right total adrenalectomy (photograph of mass shown) and was able to be tapered off her BP medications.
References
-
- Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol. 2000 Jul;183(1):S1–S22. - PubMed
-
- Berg CJ, Callaghan WM, Syverson C, Henderson Z. Pregnancy-related mortality in the United States, 1998 to 2005. Obstet Gynecol. 2010 Dec;116(6):1302–1309. - PubMed
-
- Ayala DE, Hermida RC. Ambulatory Blood Pressure Monitoring for the Early Identification of Hypertension in Pregnancy. Chronobiol Int. 2012 Sep 24; - PubMed
-
- Hermida RC, Ayala DE, Mojon A, et al. Blood pressure excess for the early identification of gestational hypertension and preeclampsia. Hypertension. 1998 Jan;31(1):83–89. - PubMed
-
- Vollebregt KC, Gisolf J, Guelen I, Boer K, van Montfrans G, Wolf H. Limited accuracy of the hyperbaric index, ambulatory blood pressure and sphygmomanometry measurements in predicting gestational hypertension and preeclampsia. J Hypertens. 2010 Jan;28(1):127–134. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
