

National surgical quality improvement program underestimates the risk associated with mild and moderate postoperative acute kidney injury
- PMID: 23928835
- PMCID: PMC3812338
- DOI: 10.1097/CCM.0b013e31829860fc
National surgical quality improvement program underestimates the risk associated with mild and moderate postoperative acute kidney injury
Abstract
Objectives: In a single-center cohort of surgical patients, we assessed the association between postoperative change in serum creatinine and adverse outcomes and compared the American College of Surgeons National Surgical Quality Improvement Program's definition for acute kidney injury with consensus risk, injury, failure, loss, and end-stage kidney and Kidney Disease: Improving Global Outcomes definitions.
Design: Retrospective single-center cohort.
Setting: Academic tertiary medical center.
Patients: Twenty-seven thousand eight hundred forty-one adult patients with no previous history of chronic kidney disease undergoing major surgery.
Interventions: Risk, injury, failure, loss, and end-stage kidney defines acute kidney injury as change in serum creatinine greater than or equal to 50% while Kidney Disease: Improving Global Outcomes uses 0.3 mg/dL change from the reference serum creatinine. Since National Surgical Quality Improvement Program defines acute kidney injury as serum creatinine change greater than 2 mg/dL, it may underestimate the risk associated with less severe acute kidney injury.
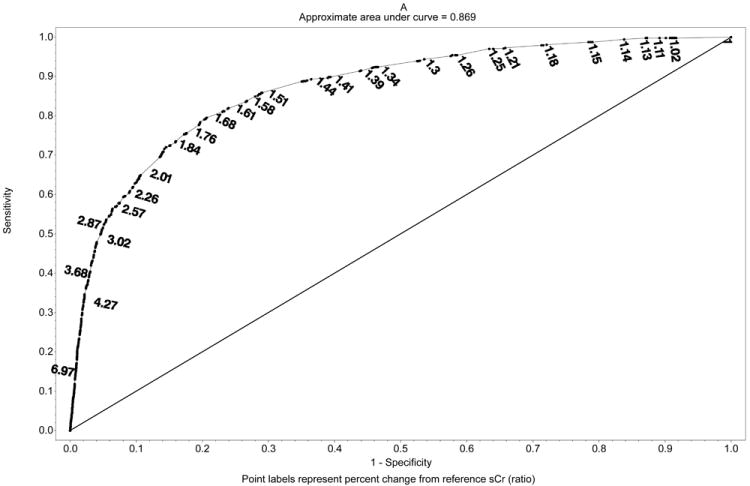
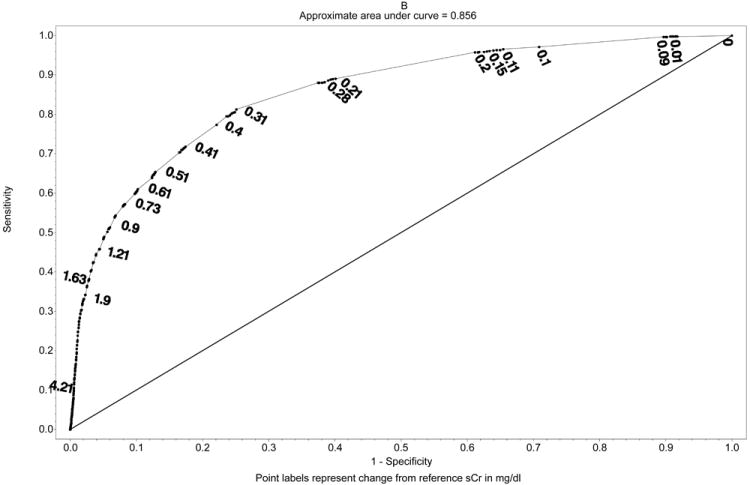
Measurements and main results: The optimal discrimination limits for both percent and absolute serum creatinine changes were calculated by maximizing sensitivity and specificity along the receiver operating characteristic curves for postoperative complications and mortality. Although prevalence of risk, injury, failure, loss, and end-stage kidney-acute kidney injury was 37%, only 7% of risk, injury, failure, loss, and end-stage kidney-acute kidney injury patients would be diagnosed with acute kidney injury using the National Surgical Quality Improvement Program definition. In multivariable logistic models, patients with risk, injury, failure, loss, and end-stage kidney or Kidney Disease: Improving Global Outcomes-acute kidney injury had a 10 times higher odds of dying compared to patients without acute kidney injury. The optimal discrimination limits for change in serum creatinine associated with adverse postoperative outcomes were as low as 0.2 mg/dL while the National Surgical Quality Improvement Program discrimination limit of 2.0 mg/dL had low sensitivity (0.05-0.28).
Conclusions: Current American College of Surgeons National Surgical Quality Improvement Program definition underestimates the risk associated with mild and moderate acute kidney injury otherwise captured by the consensus risk, injury, failure, loss, and end-stage kidney and Kidney Disease: Improving Global Outcomes criteria.
Figures
References
-
- Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–818. - PubMed
-
- Ricci Z, Cruz D, Ronco C. The RIFLE criteria and mortality in acute kidney injury: A systematic review. Kidney Int. 2008;73(5):538–546. - PubMed
-
- Hoste EA, Schurgers M. Epidemiology of acute kidney injury: How big is the problem? Crit Care Med. 2008;36(4):S146–S151. - PubMed
-
- Barrantes F, Tian J, Vazquez R, et al. Acute kidney injury criteria predict outcomes of critically ill patients. Crit Care Med. 2008;36(5):1397–1403. - PubMed
-
- Arnaoutakis GJ, Bihorac A, Martin TD, et al. RIFLE criteria for acute kidney injury in aortic arch surgery. J Thorac Cardiovasc Surg. 2007;134(6):1554–1561. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
