

Abdominal pain in ulcerative colitis
- PMID: 23929261
- PMCID: PMC3749243
- DOI: 10.1097/MIB.0b013e31829614c6
Abdominal pain in ulcerative colitis
Abstract
Background: Chronic pain is common in patients with inflammatory bowel disease and often attributed to inflammation. However, many patients with inflammatory bowel disease without evidence of active disease continue to experience pain. This study was undertaken to determine the prevalence of pain in patients with ulcerative colitis (UC) and examine the role of inflammation and psychiatric comorbidities in patients with UC with pain.
Methods: We performed a retrospective cross-sectional analysis of adult patients with UC seen at a tertiary referral inflammatory bowel disease center. Age, gender, disease duration and extent, abdominal pain rating, quality of life, physician global assessment, endoscopic and histological rating of disease severity, C reactive protein, and erythrocyte sedimentation rate were abstracted.
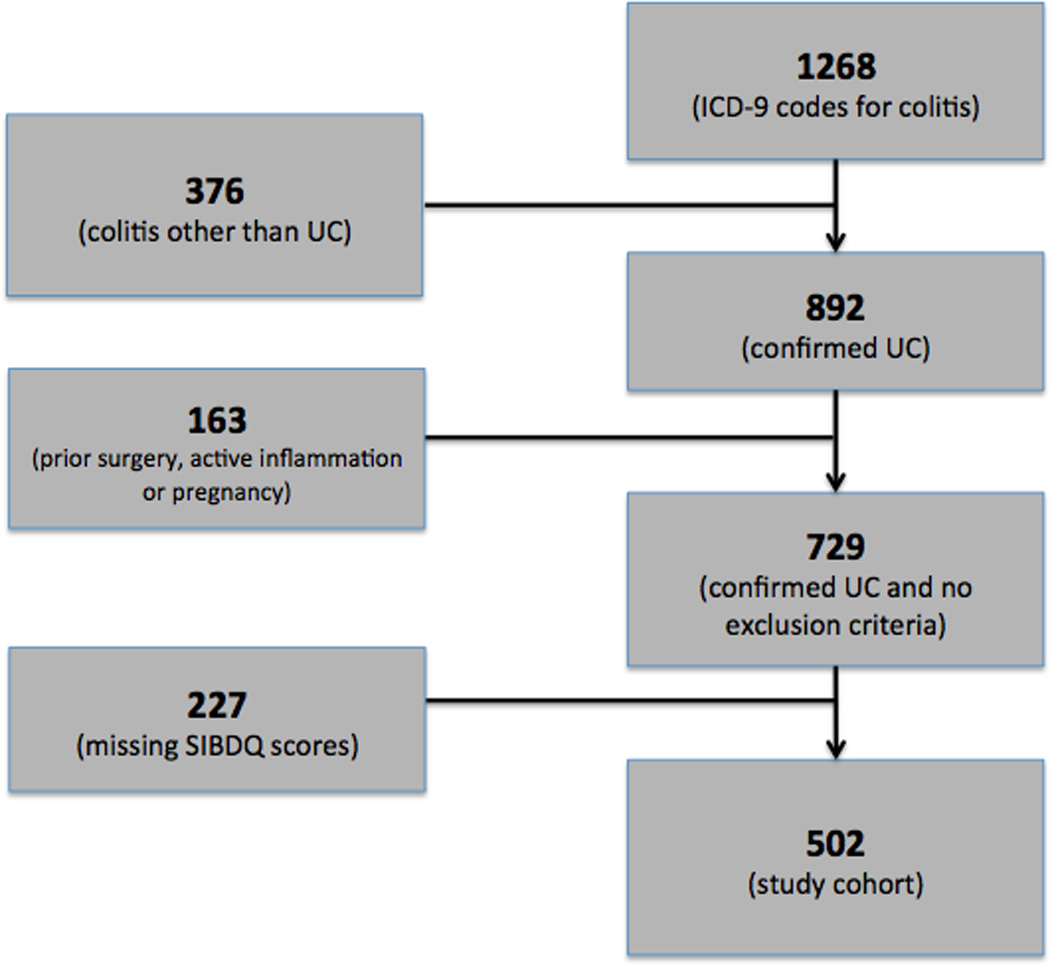
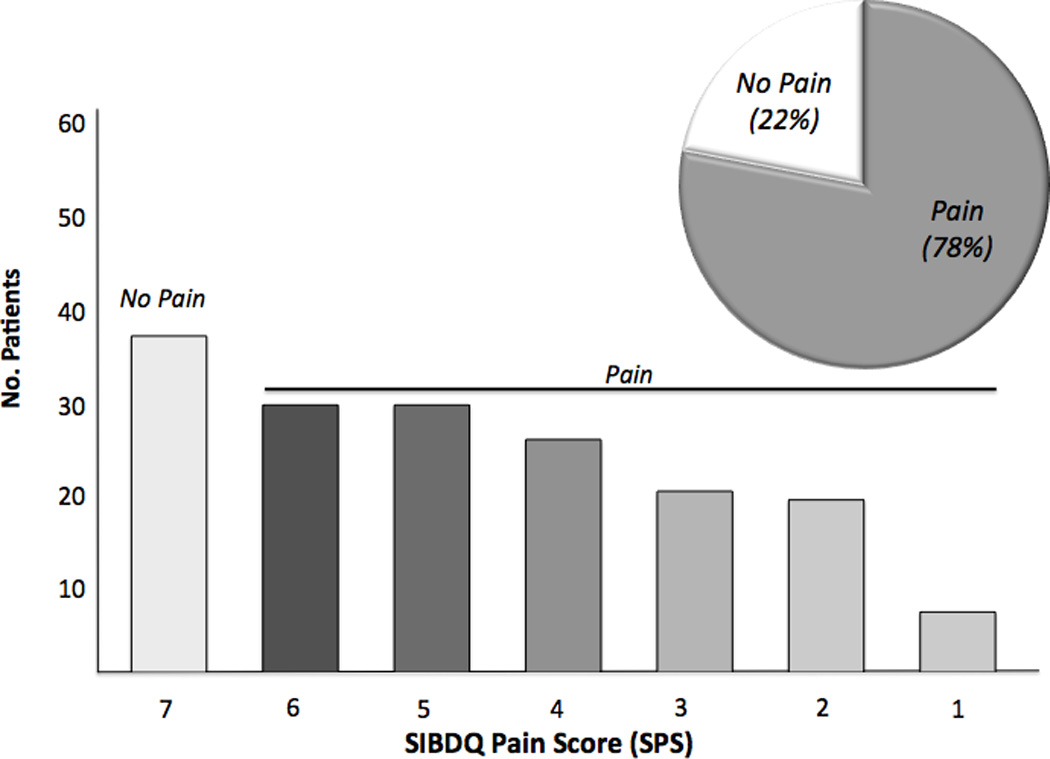
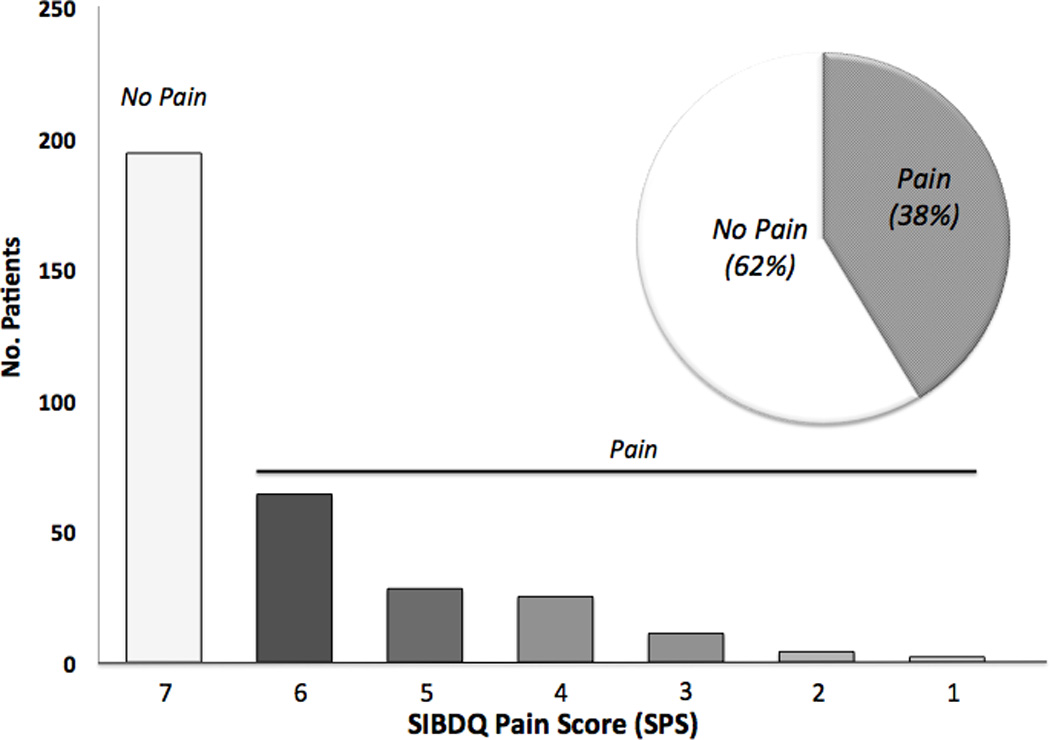
Results: A total of 1268 patients were identified using billing codes for colitis. Five hundred and two patients (48.2% women) met all inclusion criteria. Two hundred and sixty-two individuals (52.2%) complained of abdominal pain, with 108 individuals (21.5%) describing more frequent pain ("some of the time or more"). Of those with quiescent disease (n = 326), 33 patients (10%) complained of more frequent pain. Physician global assessment, endoscopic and histological severity rating, erythrocyte sedimentation rate, and C reactive protein significantly correlated with pain ratings. The best predictors of pain were physician global assessment, C reactive protein and erythrocyte sedimentation rate, female gender, and coexisting mood disorders.
Conclusions: Abdominal pain affects more than 50% of patients with UC. Although inflammation is important, the skewed gender distribution and correlation with mood disorders highlight parallels with functional bowel disorders and suggest a significant role for central mechanisms. Management strategies should thus go beyond a focus on inflammation and also include interventions that target psychological mechanisms of pain.
Figures

References
-
- Hay AR, Hay JW. Inflammatory bowel disease: medical cost algorithms. J Clin Gastroenterol. 1992;14:318–327. - PubMed
-
- Graff LA, Walker JR, Lix L, et al. The relationship of inflammatory bowel disease type and activity to psychological functioning and quality of life. Clin Gastroenterol Hepatol. 2006;4:1491–1501. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous