

Relation of regional fat distribution to left ventricular structure and function
- PMID: 23929898
- PMCID: PMC3931513
- DOI: 10.1161/CIRCIMAGING.113.000532
Relation of regional fat distribution to left ventricular structure and function
Abstract
Background: The relation of body fat distribution to left ventricular (LV) structure and function is poorly defined.
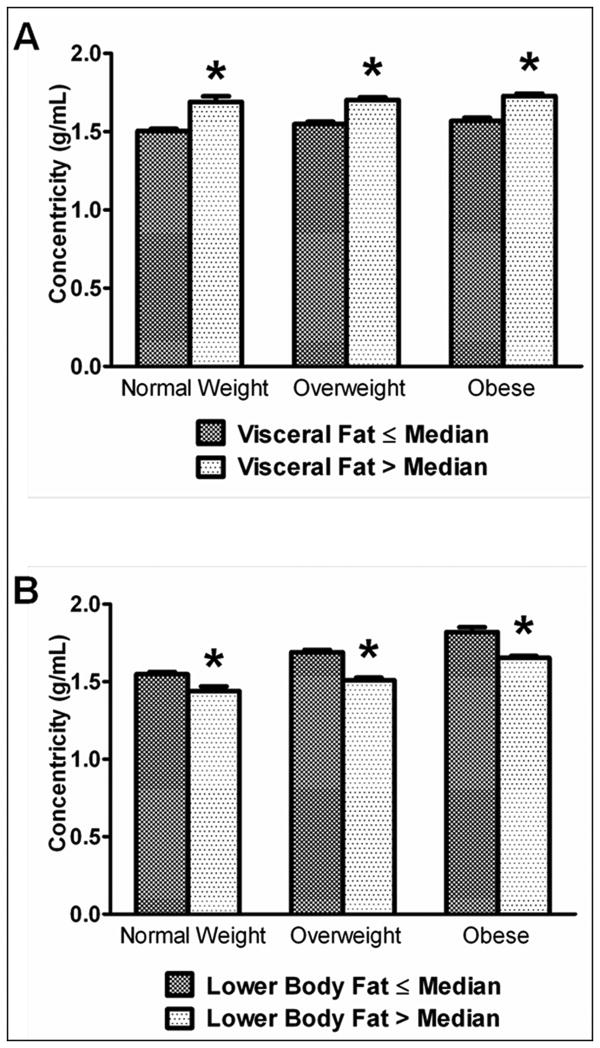
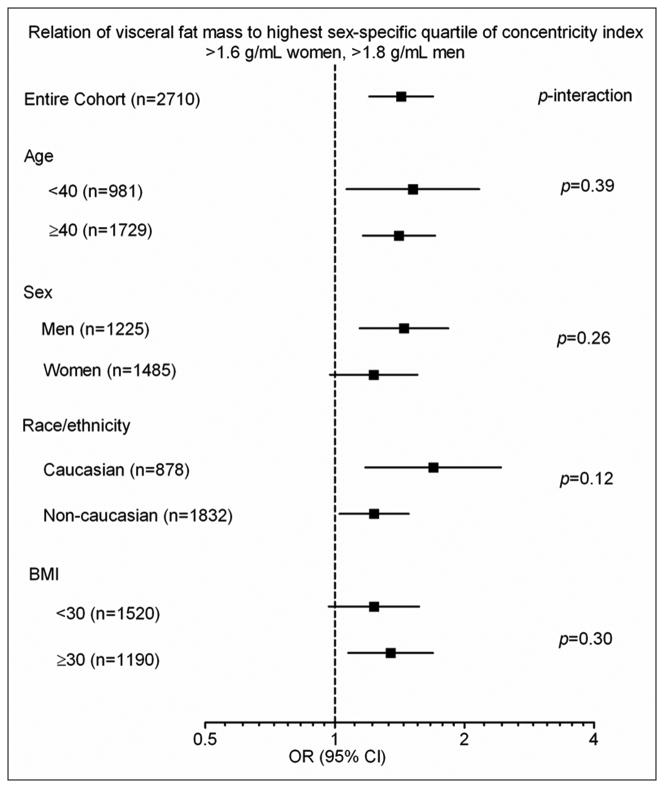
Methods and results: A total of 2710 participants without heart failure or LV dysfunction in the Dallas Heart Study underwent dual energy x-ray absorptiometry and MRI assessment of fat distribution, LV morphology, and hemodynamics. Cross-sectional associations of fat distribution with LV structure and function were examined after adjustment for age, sex, race, comorbidities, and lean mass. Mean age was 44 years with 55% women; 48% blacks; and 44% obese. After multivariable adjustment, visceral adipose tissue was associated with concentric remodeling characterized by lower LV end-diastolic volume (β=-0.21), higher concentricity (β=0.20), and wall thickness (β=0.09; P<0.0001 for all). In contrast, lower body subcutaneous fat was associated with higher LV end-diastolic volume (β=0.48), reduced concentricity (β=-0.50), and wall thickness (β=-0.28, P<0.0001 for all). Visceral adipose tissue was also associated with lower cardiac output (β=-0.10, P<0.05) and higher systemic vascular resistance (β=0.08, P<0.05), whereas lower body subcutaneous fat associated with higher cardiac output (β=0.20, P<0.0001) and lower systemic vascular resistance (β=-0.18, P<0.0001). Abdominal subcutaneous fat showed weaker associations with concentric remodeling and was not associated with hemodynamics. Among the subset of obese participants, visceral adipose tissue, but not abdominal subcutaneous fat, was significantly associated with concentric remodeling.
Conclusions: Visceral adipose tissue, a marker of central adiposity, was independently associated with concentric LV remodeling and adverse hemodynamics. In contrast, lower body subcutaneous fat was associated with eccentric remodeling. The impact of body fat distribution on heart failure risk requires prospective study.
Keywords: body fat distribution; concentric remodeling; hypertrophy, left ventricular; intra-abdominal fat; obesity.
Conflict of interest statement
Figures
References
-
- Heckbert SR, Post W, Pearson GD, Arnett DK, Gomes AS, Jerosch-Herold M, Hundley WG, Lima JA, Bluemke DA. Traditional cardiovascular risk factors in relation to left ventricular mass, volume, and systolic function by cardiac magnetic resonance imaging: the Multiethnic Study of Atherosclerosis. J Am Coll Cardiol. 2006;48:2285–92. - PMC - PubMed
-
- Lauer MS, Anderson KM, Kannel WB, Levy D. The impact of obesity on left ventricular mass and geometry. The Framingham Heart Study. JAMA. 1991;266:231–6. - PubMed
-
- Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, Kannel WB, Vasan RS. Obesity and the risk of heart failure. N Engl J Med. 2002;347:305–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
