

Fibroblast growth factor 23 and cardiovascular mortality after kidney transplantation
- PMID: 23929933
- PMCID: PMC3817902
- DOI: 10.2215/CJN.01880213
Fibroblast growth factor 23 and cardiovascular mortality after kidney transplantation
Abstract
Background and objectives: Circulating fibroblast growth factor 23 (FGF23) is associated with adverse cardiovascular outcomes in CKD. Whether FGF23 predicts cardiovascular mortality after kidney transplantation, independent of measures of mineral metabolism and cardiovascular risk factors, is unknown.
Design, setting, participants, & measurements: The association between plasma C-terminal FGF23 and cardiovascular mortality was analyzed in a single-center prospective cohort of 593 stable kidney transplant recipients (mean age ± SD, 52 ± 12 years; 54% male; estimated GFR, 47 ± 16 ml/min per 1.73 m(2)), at a median of 6.1 (interquartile range, 2.7-11.7) years after transplantation. Multivariate Cox regression models were built, adjusting for measures of renal function and mineral metabolism; Framingham risk factors; the left ventricular wall strain markers midregional fragment of pro-A-type natriuretic peptide (MR-proANP) and N-terminal-pro brain natriuretic peptide (NT-proBNP); and copeptin, the stable C-terminal portion of the precursor of vasopressin.
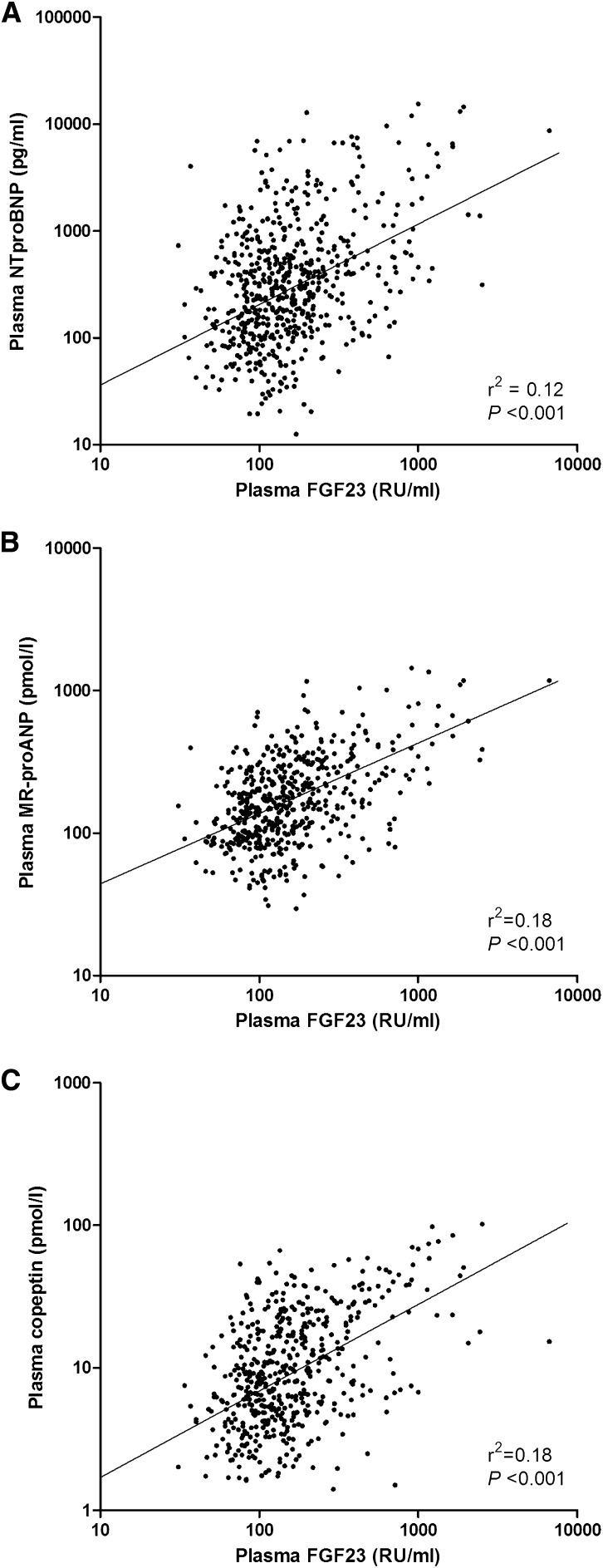
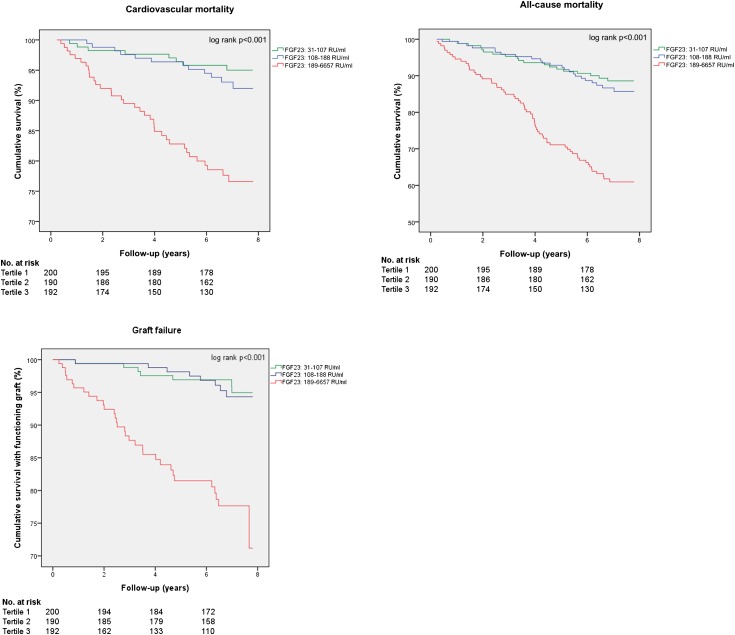
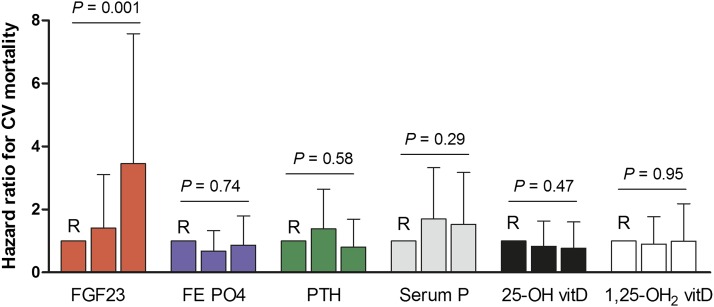
Results: In multivariate linear regression analysis, MR-proANP (β=0.20, P<0.001), NT-proBNP (β=0.18, P<0.001), and copeptin (β=0.26, P<0.001) were independently associated with FGF23. During follow-up for 7.0 (interquartile range, 6.2-7.5) years, 128 patients (22%) died, of whom 66 (11%) died due to cardiovascular disease; 54 (9%) had graft failure. FGF23 was associated with an higher risk of cardiovascular mortality in a fully adjusted multivariate Cox regression model (hazard ratio [HR], 1.88 [95% confidence interval (CI), 1.11 to 3.19]; P=0.02). FGF23 was also independently associated with all-cause mortality (full model HR, 1.86 [95% CI, 1.27 to 2.73]; P=0.001). Net reclassification improved for both cardiovascular mortality (HR, 0.07 [95% CI, 0.01 to 0.14]; P<0.05) and all-cause mortality (HR, 0.11 [95% CI, 0.05 to 0.18]; P<0.001).
Conclusions: Plasma FGF23 is independently associated with cardiovascular and all-cause mortality after kidney transplantation. The association remained significant after adjustment for measures of mineral metabolism and cardiovascular risk factors.
Figures
References
-
- Jardine AG, Gaston RS, Fellstrom BC, Holdaas H: Prevention of cardiovascular disease in adult recipients of kidney transplants. Lancet 378: 1419–1427, 2011 - PubMed
-
- Larsson T, Nisbeth U, Ljunggren O, Jüppner H, Jonsson KB: Circulating concentration of FGF-23 increases as renal function declines in patients with chronic kidney disease, but does not change in response to variation in phosphate intake in healthy volunteers. Kidney Int 64: 2272–2279, 2003 - PubMed
-
- Ärnlöv J, Carlsson AC, Sundström J, Ingelsson E, Larsson A, Lind L, Larsson TE: Higher fibroblast growth factor-23 increases the risk of all-cause and cardiovascular mortality in the community. Kidney Int 83: 160–166, 2013 - PubMed
-
- Kestenbaum B, Sampson JN, Rudser KD, Patterson DJ, Seliger SL, Young B, Sherrard DJ, Andress DL: Serum phosphate levels and mortality risk among people with chronic kidney disease. J Am Soc Nephrol 16: 520–528, 2005 - PubMed
-
- Fliser D, Kollerits B, Neyer U, Ankerst DP, Lhotta K, Lingenhel A, Ritz E, Kronenberg F, Kuen E, König P, Kraatz G, Mann JF, Müller GA, Köhler H, Riegler P, MMKD Study Group : Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: The Mild to Moderate Kidney Disease (MMKD) Study. J Am Soc Nephrol 18: 2600–2608, 2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
