

A contemporary analysis of morbidity and outcomes in cytoreduction/hyperthermic intraperitoneal chemoperfusion
- PMID: 23930210
- PMCID: PMC3699845
- DOI: 10.1002/cam4.80
A contemporary analysis of morbidity and outcomes in cytoreduction/hyperthermic intraperitoneal chemoperfusion
Abstract
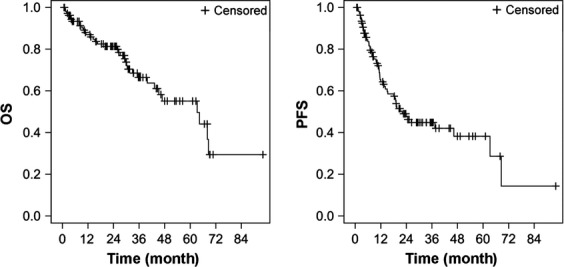
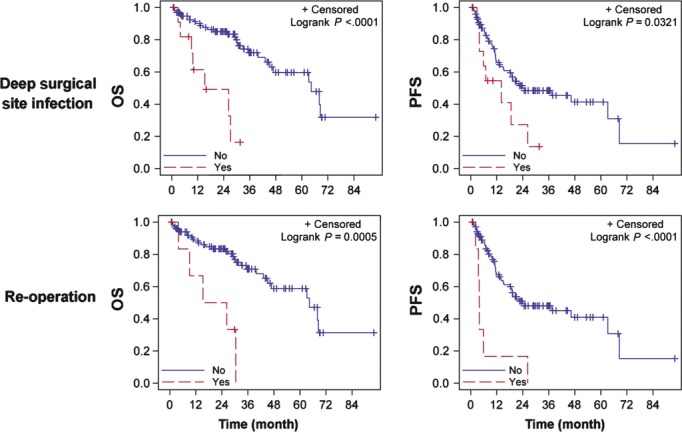
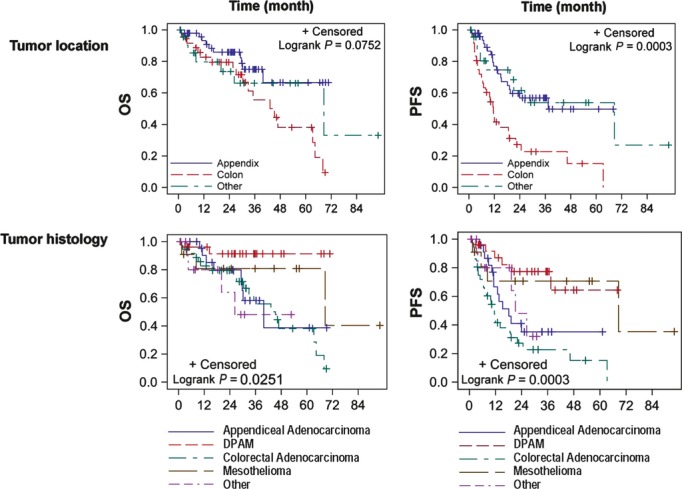
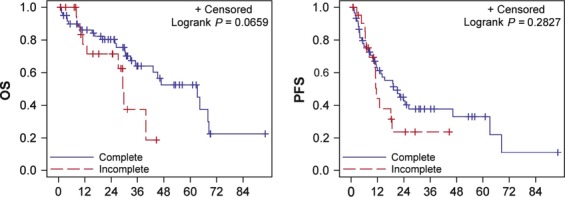
The risks and benefits of cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (CS/HIPEC) continue to be debated by the oncology community. A retrospective analysis of contemporary data (2003-2011) was performed to provide objective information regarding surgical morbidity, mortality, and survival for patients undergoing CS/HIPEC at a comprehensive cancer center. While procedure-associated morbidity was comparable to other major surgical oncology procedures, there was no operative or 30-day mortality and 60-day mortality was 2.7%. Increasing numbers of bowel resections were found to correlate to an increased incidence of deep surgical site infections (including abscess and enterocutaneous fistula) and need for reoperation which was in turn associated with a decreased overall survival (OS) and progression-free survival (PFS). Five-year OS rates varied by site of tumor origin and histology (disseminated peritoneal adenomucinosis [91.3%], Mesothelioma [80.8%], Appendiceal Adenocarcinoma [38.7%], and Colorectal Adenocarcinoma [38.2%]). With an acceptable morbidity and mortality rate, CS/HIPEC should be included as an effective treatment modality in the multidisciplinary care of select patients with peritoneal metastases.
Keywords: Carcinomatosis; HIPEC; colorectal cancer; cytoreduction; morbidity.
Figures
References
-
- Chu DZ, Lang NP, Thompson C, Osteen PK, Westbrook KC. Peritoneal carcinomatosis in nongynecologic malignancy. A prospective study of prognostic factors. Cancer. 1989;63:364–367. - PubMed
-
- Sadeghi B, Arvieux C, Glehen O, Beaujard AC, Rivoire M, Baulieux J, et al. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer. 2000;88:358–363. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
