

Microbubble transmission during cardiotomy infusion of a hardshell venous reservoir with integrated cardiotomy versus a softshell venous reservoir with separated cardiotomy: an in vitro comparison
- PMID: 23930376
- PMCID: PMC4557584
Microbubble transmission during cardiotomy infusion of a hardshell venous reservoir with integrated cardiotomy versus a softshell venous reservoir with separated cardiotomy: an in vitro comparison
Abstract
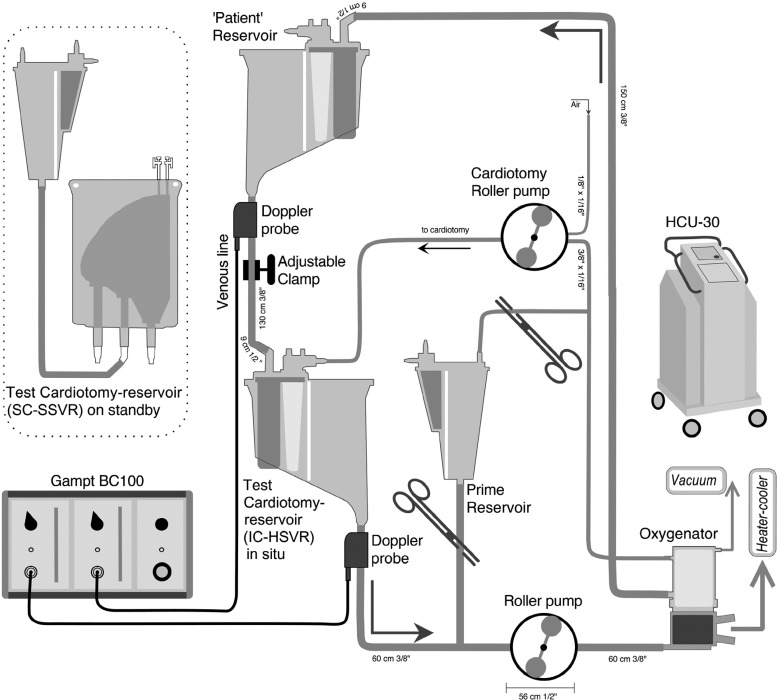
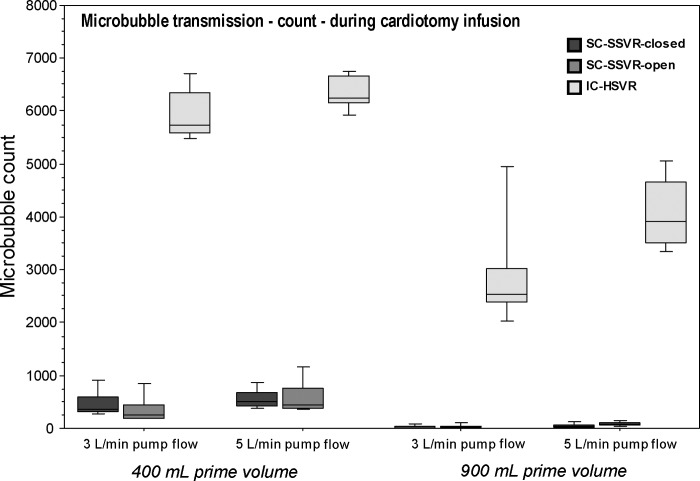
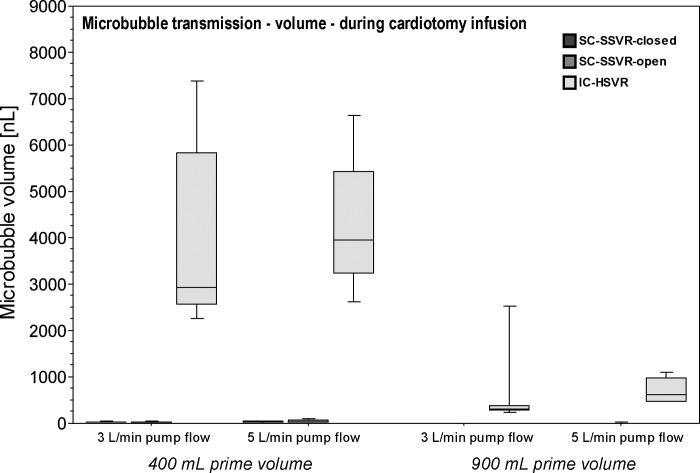
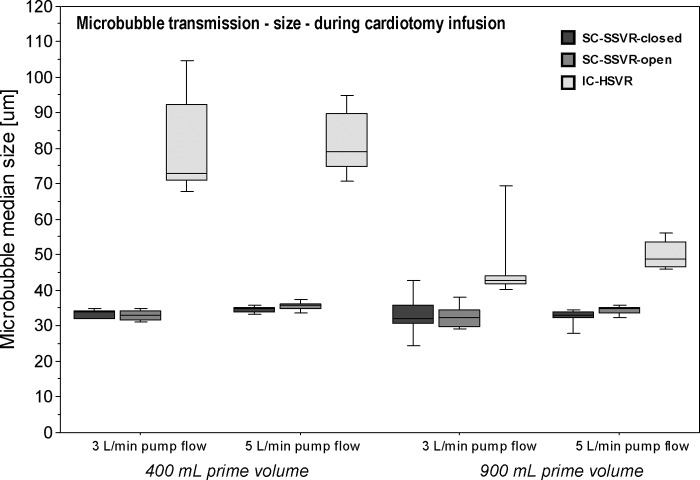
An important mechanism for postoperative cognitive impairment after cardiac surgery using cardiopulmonary bypass (CPB) is microemboli. One component of the CPB circuit-the cardiotomy-is a major source of gaseous microemboli because it aspirates significant volumes of air with blood from the operative field and intracardiac chambers. Cardiotomies are either integrated within an open hardshell venous reservoir (IC-HSVR) or are a separate canister attached to a softshell collapsible venous reservoir bag (SC-SSVR). The purpose of this study was to compare the Medtronic IC-HSVR (Affinity NT CVR) with Medtronic's SC-SSVR (CB 1351, CBMVR 1600) in terms of relative microbubble transmission during cardiotomy infusion. A recirculating in vitro circuit primed with blood was used to compare the two cardiotomy-reservoir systems with the venous reservoir in the SC-SSVR further assessed in a fully closed or partially open state (SC-SSVR-closed; SC-SSVR-open). Microbubbles were detected using a GAMPT BC100 Doppler system in the outflow line of the venous reservoir. Measurements were taken before (baseline) and after aerated prime was pumped into the cardiotomy while altering pump flow rates (3 L/min; 5 L/min) and reservoir prime volumes (400 mL; 900 mL). Infusing cardiotomy blood into the venous reservoir was associated with an increase in microbubbles and bubble volume transmitted by both cardiotomy-reservoir systems with the magnitude rising with reduced prime volumes. The effect was markedly greater with the IC-HSVR. The IC-HSVR also transmitted larger bubbles, particularly with reduced prime volumes. There was no significant difference in microbubble transmission seen between the SC-SSVR-closed and SC-SSVR-open. The SC-SSVR transmits fewer microbubbles than the IC-HSVR during cardiotomy infusion and should be considered as the preferential system. Because both cardiotomy-reservoir systems transmitted microbubbles during cardiotomy infusion, particularly at the lower venous reservoir volume, it is important to use strategies to minimize cardiotomy microbubble infusion.
Conflict of interest statement
The senior author has stated that the authors have reported no material, financial, or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures
References
-
- Lee R, Li S, Rankin S, et al. Fifteen-year outcome trends for valve surgery in North America. Ann Thorac Surg. 2011;91:677–684. - PubMed
-
- McKhann GM, Grega MA, Borowicz LM, Baumgartner WA, Selnes OA.. Stroke and encephalopathy after cardiac surgery an update. Stroke. 2006;37:562–571. - PubMed
-
- Fearn SJ, Pole R, Wesnes K, Faragher EB, Hooper TL, McCollum CN.. Cerebral injury during cardiopulmonary bypass: Emboli impair memory. J Thorac Cardiovasc Surg. 2001;121:1150–1160. - PubMed
-
- Likosky DS, Roth RM, Saykin AJ, Eskey CJ, Ross CS, O’Connor GT.. Neurological injury associated with CABG surgery: Outcomes, mechanisms, and opportunities for improvement. Heart Surg Forum. 2004;7:650–661. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials