

Case Reports
doi: 10.1016/j.jcjo.2013.01.014.
Scleral penetration of an unusually aggressive case of a retinal hemangioblastoma
- PMID: 23931485
- PMCID: PMC4005102
- DOI: 10.1016/j.jcjo.2013.01.014
Item in Clipboard
Case Reports
Scleral penetration of an unusually aggressive case of a retinal hemangioblastoma
Can J Ophthalmol.
2013 Aug.
No abstract available
Figures
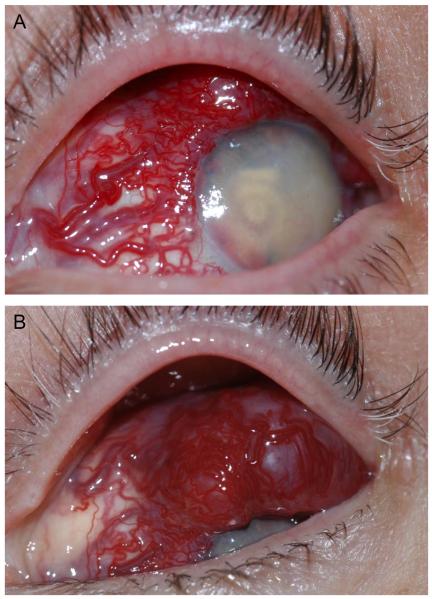
External photos of the highly vascularized lesion. A. Dilated tortuous vessels involving the nasal, superior, and temporal conjunctiva feed a highly vascularized subconjunctival lesion. The cornea is translucent; there is florid neovascularization with a layered hyphema in the anterior chamber. B. Views of the superior conjunctiva reveal that the lesion overrides the corneal limbus superiorly.
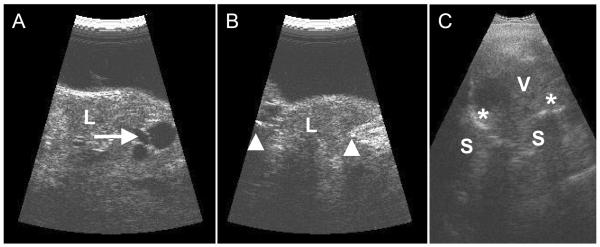
Ultrasound exam of the vascularized lesion. A. and B. Transverse (cross-section; A) and longitudinal (radial section; B) images using a 20 MHz probe (using a fluid standoff) of the anterior segment reveals that the lesion (L) on the outer surface of the globe is highly reflective with low reflective areas consistent with vessels and/or cystic spaces (arrow); the lesion protrudes through the sclera (arrow heads). C. Contact B-scan (10 MHz) showing the disorganized intraocular structures (V) and the marked calcification of the globe wall (asterick) with the associated acoustic shadowing (S).
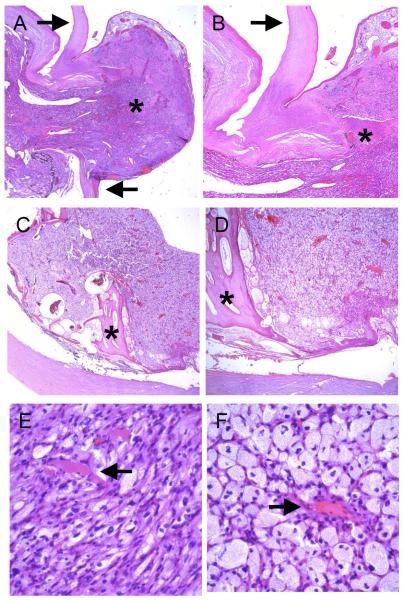
Microscopic examination. A. and B. The highly vascularized intraocular lesion extended through a defect in the superior limbus (arrows) and formed an extraocular mass (asterisk, original magnifications 20X and 40X). The lesion was covered by conjunctival epithelium. C. and D. The tumor largely replaced the retina and choroid, and bony RPE metaplasia was noted in the posterior portion of the globe (asterisks, original magnifications 20X and 40X). E and F. The hemangioblastoma was composed of thin-walled, capillary-like blood vessels (arrows) and numerous lipidized stromal (tumor) cells (original magnification 400X).
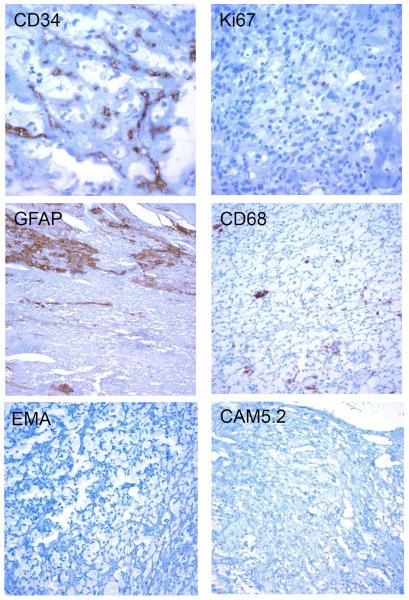
Immunohistochemical analysis. The lesion contained numerous small vessels that stained positive for the endothelial marker CD34. The lipidized stromal (tumor) cells had a low proliferation index, as demonstrated by only rare Ki67 positive cells. There were entrapped glial elements (GFAP) and rare macrophages (CD68). The tumor cells were immunonegative for EMA and CAM5.2. (Original magnifications 200X or 400X).
Similar articles
-
Aggressive-fungating retinal hemangioblastoma.J Cancer Res Ther. 2021 Jan-Mar;17(1):279-281. doi: 10.4103/jcrt.JCRT_718_18. J Cancer Res Ther. 2021. PMID: 33723171
-
Clinically unsuspected retinal hemangioblastoma in a blind eye as the initial manifestation of von Hippel-Lindau disease.Pathol Res Pract. 2012 Mar 15;208(3):186-8. doi: 10.1016/j.prp.2011.12.007. Epub 2012 Jan 26. Pathol Res Pract. 2012. PMID: 22281434
-
[Retinal capillary hemangioblastoma in Von Hippel-Lindau disease].J Fr Ophtalmol. 2017 Jan;40(1):80-81. doi: 10.1016/j.jfo.2016.10.006. Epub 2017 Jan 10. J Fr Ophtalmol. 2017. PMID: 28087080 French. No abstract available.
-
Haemangioblastoma, haemangioblastomatosis, and von Hippel-Lindau disease.Adv Tech Stand Neurosurg. 1993;20:197-304. doi: 10.1007/978-3-7091-6912-4_6. Adv Tech Stand Neurosurg. 1993. PMID: 8397535 Review. No abstract available.
-
Von hippel-lindau disease: a genetic and clinical review.Semin Ophthalmol. 2013 Sep-Nov;28(5-6):377-86. doi: 10.3109/08820538.2013.825281. Semin Ophthalmol. 2013. PMID: 24138046 Review.
Cited by
-
Retinal Hemangioblastoma with Extraocular Extension: Report of Three Cases.Ocul Oncol Pathol. 2021 Jun;7(3):177-181. doi: 10.1159/000512173. Epub 2021 Jan 7. Ocul Oncol Pathol. 2021. PMID: 34307328 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
