

Short-lag spatial coherence imaging of cardiac ultrasound data: initial clinical results
- PMID: 23932276
- PMCID: PMC3966558
- DOI: 10.1016/j.ultrasmedbio.2013.03.029
Short-lag spatial coherence imaging of cardiac ultrasound data: initial clinical results
Abstract
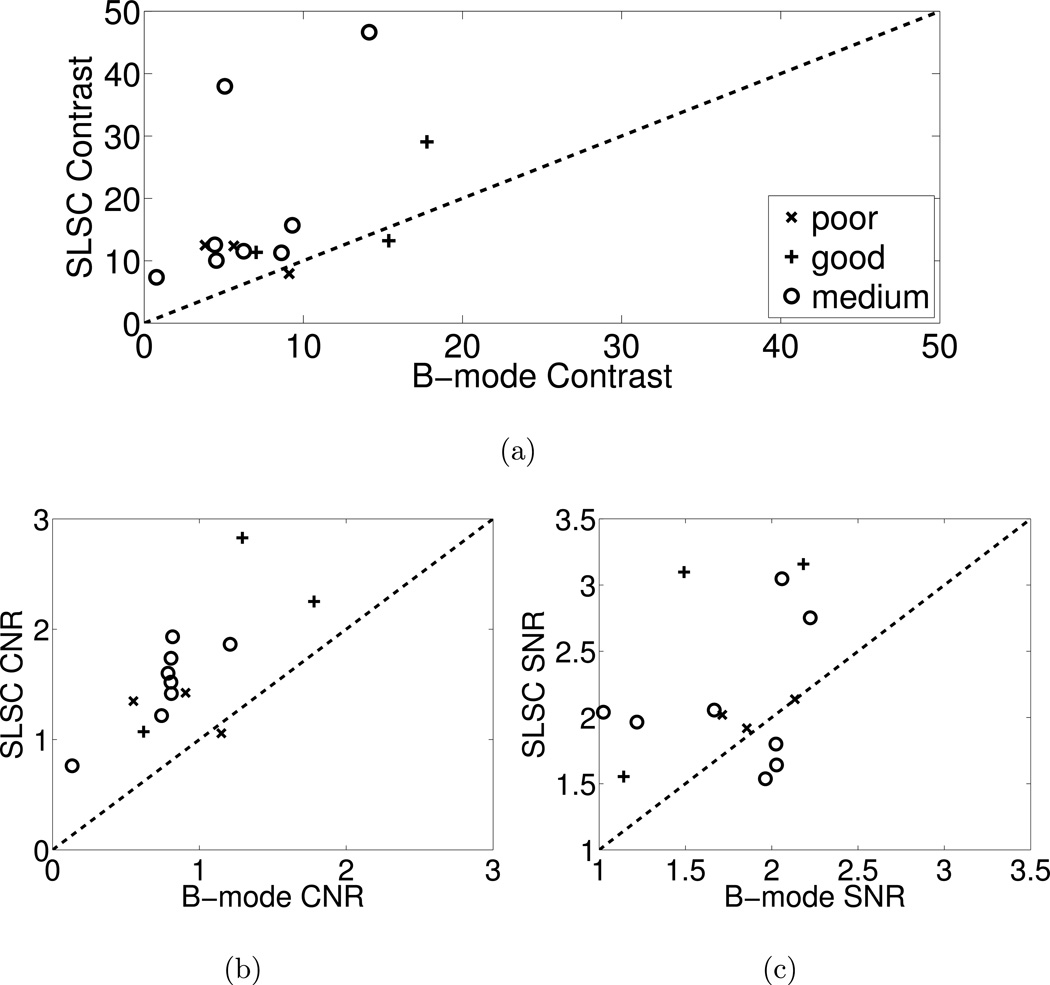
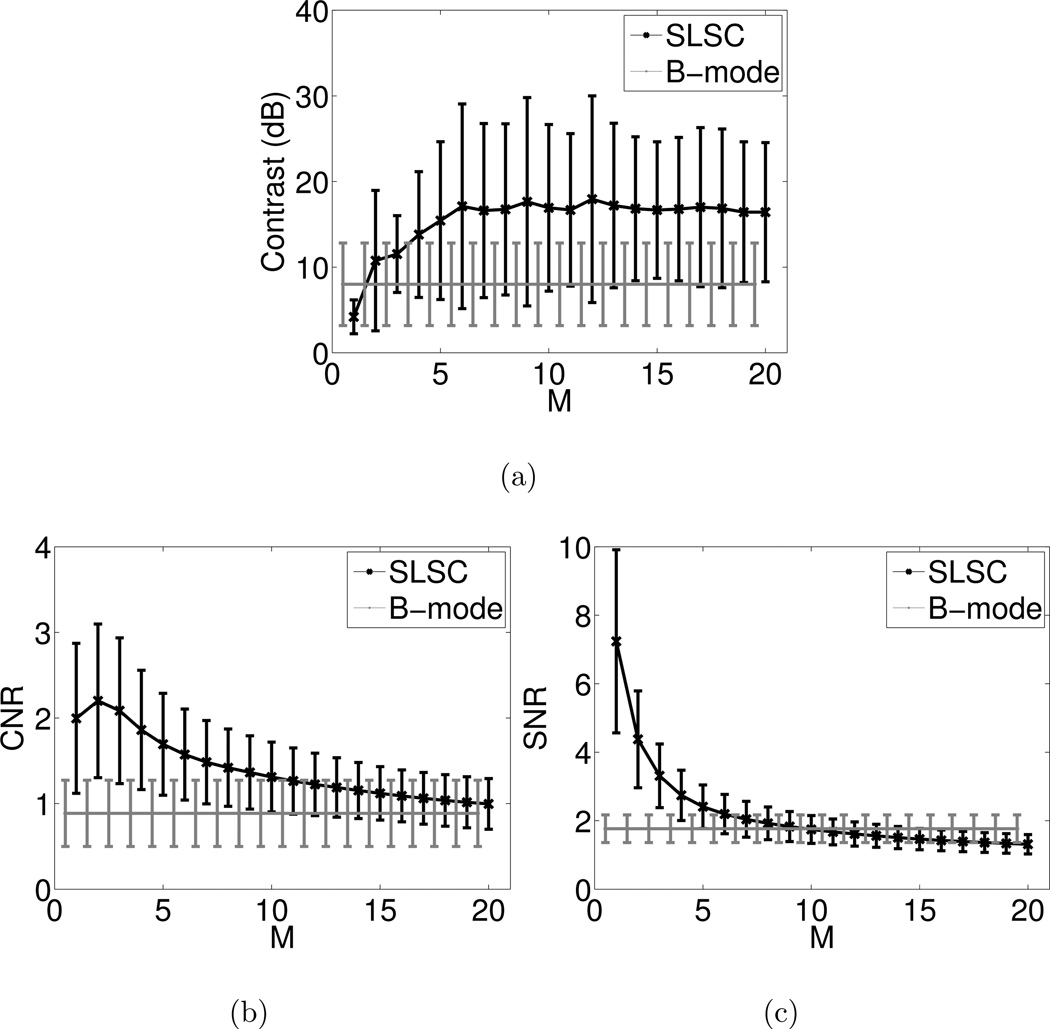
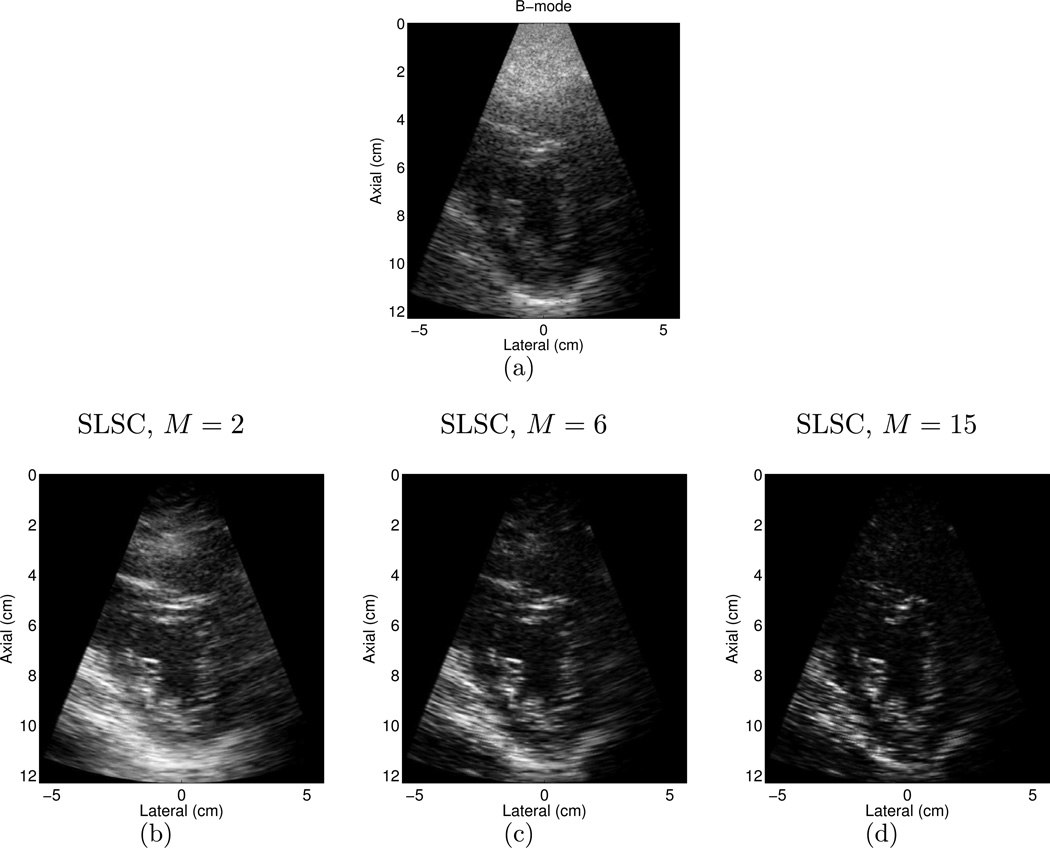
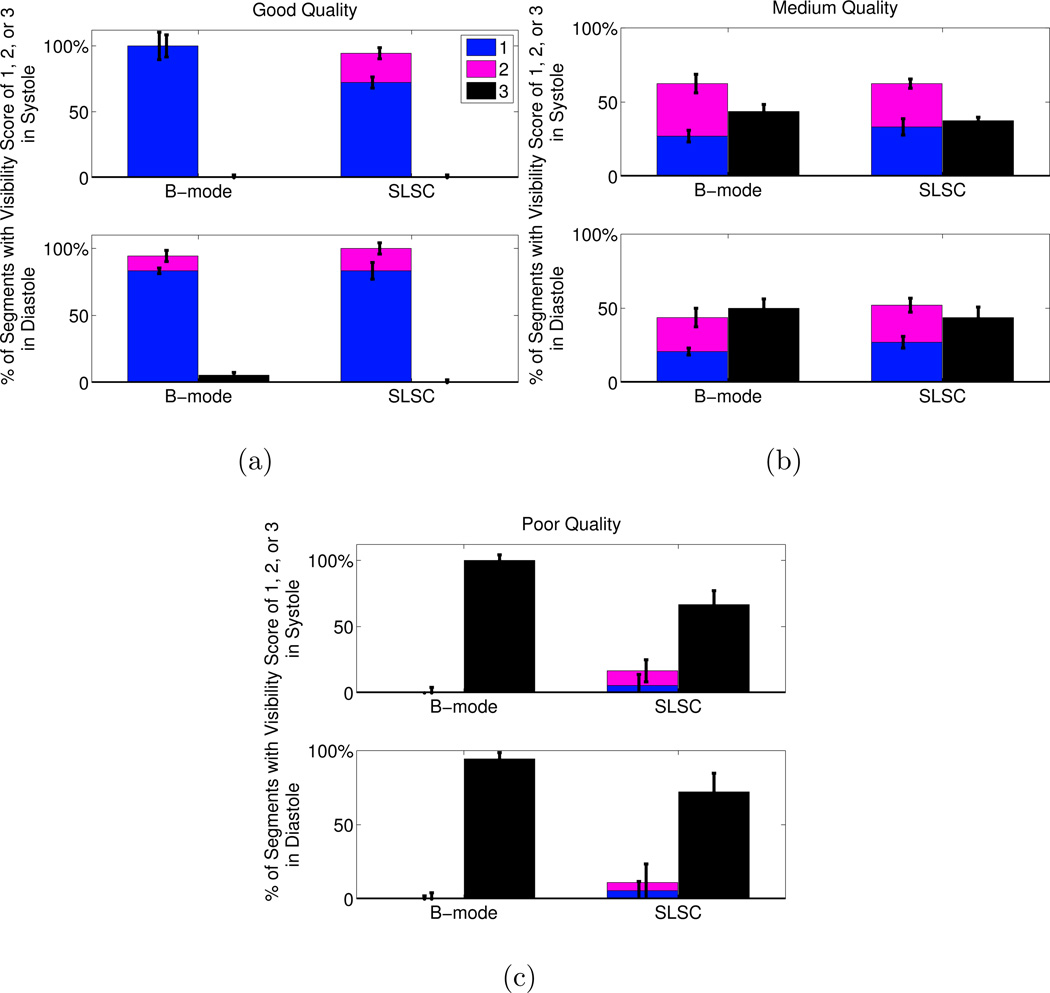
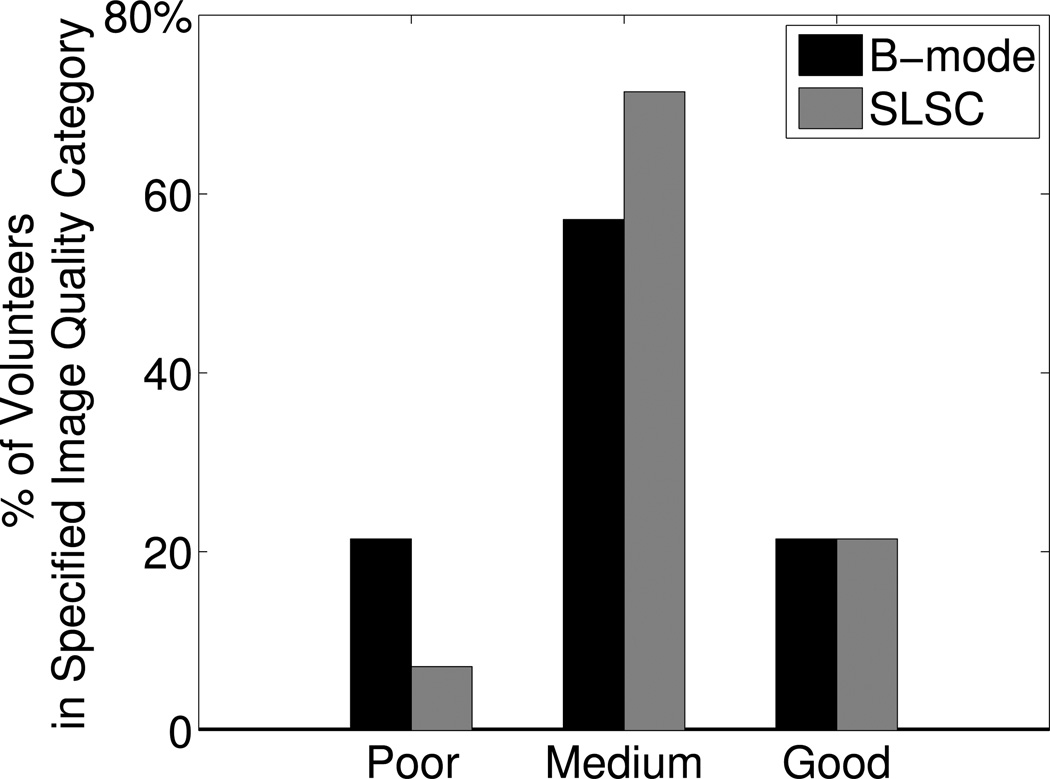
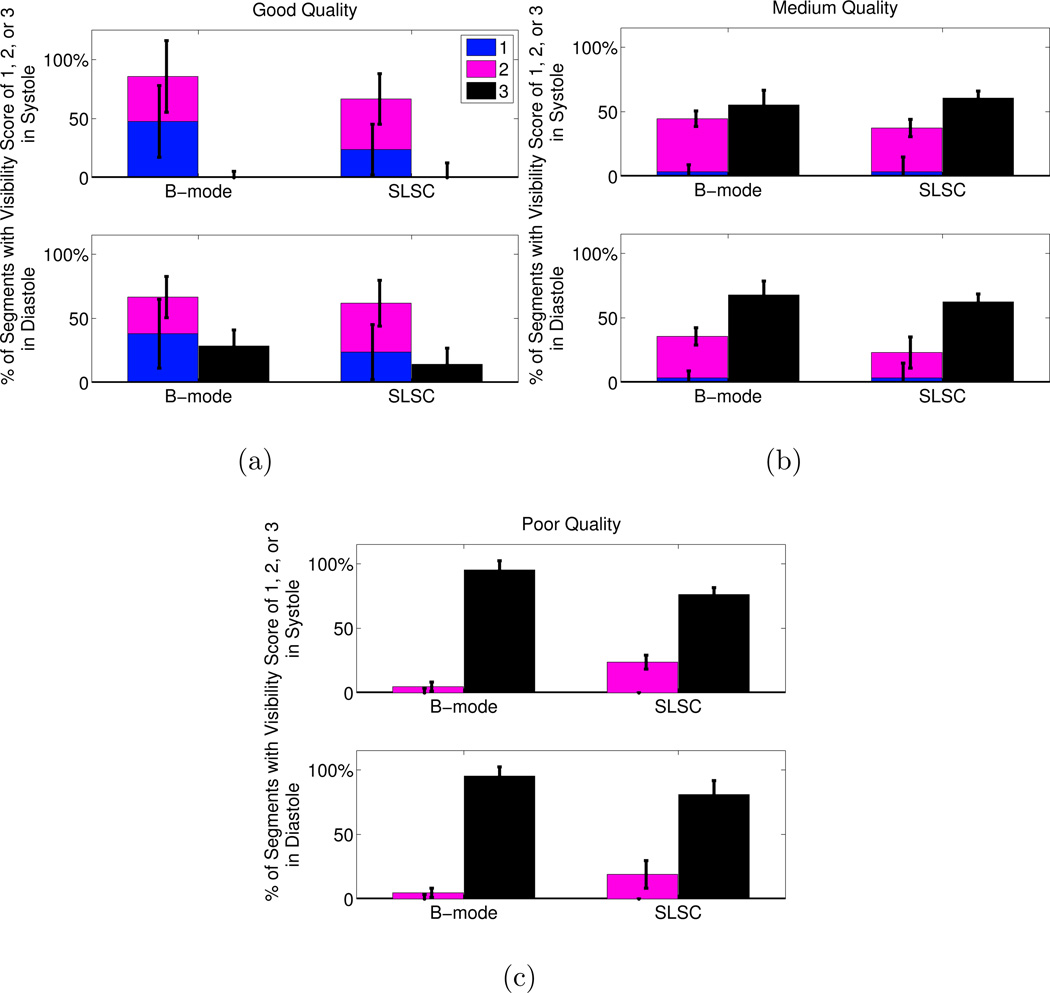
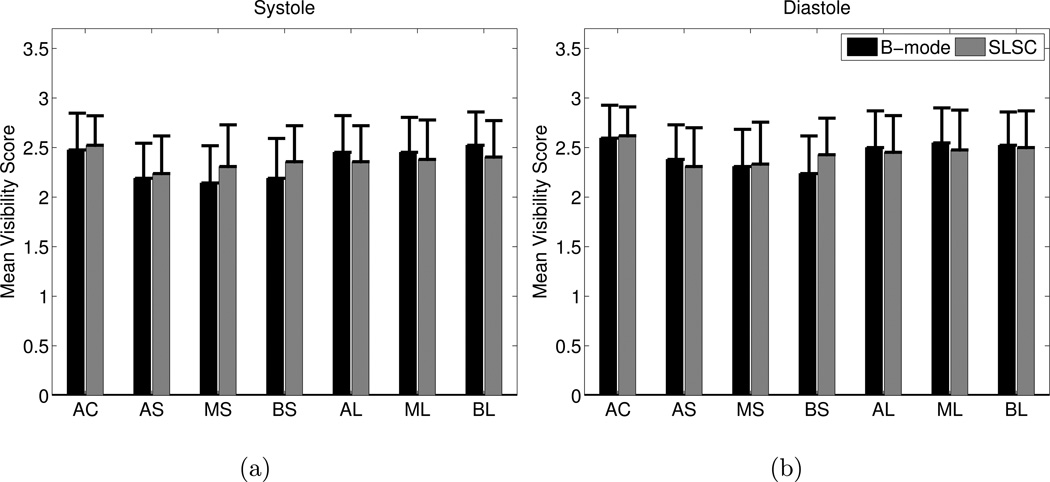
Short-lag spatial coherence (SLSC) imaging is a novel beamforming technique that reduces acoustic clutter in ultrasound images. A clinical study was conducted to investigate clutter reduction and endocardial border detection in cardiac SLSC images. Individual channel echo data were acquired from the left ventricle of 14 volunteers, after informed consent and institutional review board approval. Paired B-mode and SLSC images were created from these data. Contrast, contrast-to-noise, and signal-to-noise ratios were measured in paired images, and these metrics were improved with SLSC imaging in most cases. Three cardiology fellows rated the visibility of endocardial segments in randomly ordered B-mode and SLSC cine loops. SLSC imaging offered 22%-33% improvement (p < 0.05) in endocardial border visibility when B-mode image quality was poor (i.e., 80% or more of the endocardial segments could not be visualized by the three reviewers). The percentage of volunteers with poor-quality images was decreased from 21% to 7% with the SLSC beamformer. Results suggest that SLSC imaging has the potential to improve clinical cardiac assessments that are challenged by clutter.
Keywords: B-mode; Clutter reduction; Coherence-based beamforming; Contrast; Echocardiography; Endocardial border detection; M-mode; Signal-to-noise ratio.
2013 World Federation for Ultrasound in Medicine & Biology. Published by Elsevier Inc. All rights reserved
Figures
References
-
- Al-Mansour H, Mulvagh S, Pumper G, Klarich K, Foley D. Usefulness of harmonic imaging for left ventricular opacification and endocardial border delineation by optison. The American Journal of Cardiology. 2000;856:795–799. - PubMed
-
- Bamber J, Mucci R, Orofino D. Spatial Coherence and Beamformer Gain. Acoustical Imaging. 2000;24:43–48.
-
- Becher H, Tiemann K, Schlosser T, Pohl C, Nanda N, Averkiou M, Powers J, Luderitz B. Improvement in endocardial border delineation using tissue harmonic imaging. Echocardiography. 1998;155:511–517. - PubMed
-
- Bezante G, Rosa G, Bruni R, Chen X, Villa G, Scopinaro A, Balbi M, Barsotti A, Schwarz K. Improved assessment of left ventricular volumes and ejection fraction by contrast enhanced harmonic color Doppler echocardiography. The International Journal of Cardiovascular Imaging (formerly Cardiac Imaging) 2005;216:609–616. - PubMed
-
- Caiati C, Zedda N, Montaldo C, Montisci R, Iliceto S. Contrast-enhanced transthoracic second harmonic echo doppler with adenosine A noninvasive, rapid and effective method for coronary flow reserve assessment. Journal of the American College of Cardiology. 1999;341:122–130. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
