

Racial and ethnic health disparities in reproductive medicine: an evidence-based overview
- PMID: 23934691
- PMCID: PMC4152894
- DOI: 10.1055/s-0033-1348889
Racial and ethnic health disparities in reproductive medicine: an evidence-based overview
Abstract
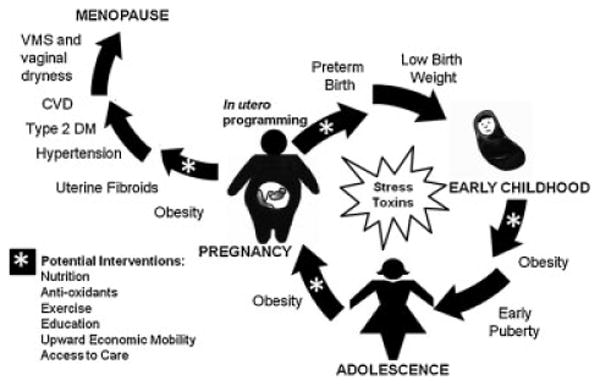
Racial and ethnic health disparities in reproductive medicine exist across the life span and are costly and burdensome to our healthcare system. Reduction and ultimate elimination of health disparities is a priority of the National Institutes of Health who requires reporting of race and ethnicity for all clinical research it supports. Given the increasing rates of admixture in our population, the definition and subsequent genetic significance of self-reported race and ethnicity used in health disparity research is not straightforward. Some groups have advocated using self-reported ancestry or carefully selected single-nucleotide polymorphisms, also known as ancestry informative markers, to sort individuals into populations. Despite the limitations in our current definitions of race and ethnicity in research, there are several clear examples of health inequalities in reproductive medicine extending from puberty and infertility to obstetric outcomes. We acknowledge that socioeconomic status, education, insurance status, and overall access to care likely contribute to the differences, but these factors do not fully explain the disparities. Epigenetics may provide the biologic link between these environmental factors and the transgenerational disparities that are observed. We propose an integrated view of health disparities across the life span and generations focusing on the metabolic aspects of fetal programming and the effects of environmental exposures. Interventions aimed at improving nutrition and minimizing adverse environmental exposures may act synergistically to reverse the effects of these epigenetic marks and improve the outcome of our future generations.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Figures
References
-
- National Institutes of Health. Bethesda, MD: National Institutes of Health; 2011. [Accessed February 12, 2013]. NIH Health Disparities Strategic Plan and Budget, Fiscal Years 2009-2013. [Online]. Available at: http://www.nimhd.nih.gov/about_ncmhd/Strategic%20Plan%20FY%202009-2013%2....
-
- National Institutes of Health. Bethesda, MD: National Institutes of Health; 2011. [Accessed February 12, 2013]. NIH Policy on Reporting Race and Ethnicity Data: Subjects in Clinical Research. [Online]. Available at: http://grants.nih.gov\grants\guide\notice-files\NOT-OD-01-053.html.
-
- U.S. Census Bureau. Statistical Abstract of the United States. 131st. Washington, DC: US Government printing office; 2012.
-
- ACOG Committee on Health Care for Underdeserved Women. ACOG committee opinion. Number 317, October 2005. Racial and ethnic disparities in women's health. Obstet Gynecol. 2005;106(4):889–892. - PubMed
-
- Keita SO, Kittles RA, Royal CD, et al. Conceptualizing human variation. Nat Genet. 2004;36(11, Suppl):S17–S20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
