

Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study
- PMID: 23935011
- PMCID: PMC6701181
- DOI: 10.1161/CIRCULATIONAHA.113.002283
Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study
Abstract
Background: Patients experiencing major bleeding while taking vitamin K antagonists require rapid vitamin K antagonist reversal. We performed a prospective clinical trial to compare nonactivated 4-factor prothrombin complex concentrate (4F-PCC) with plasma for urgent vitamin K antagonist reversal.
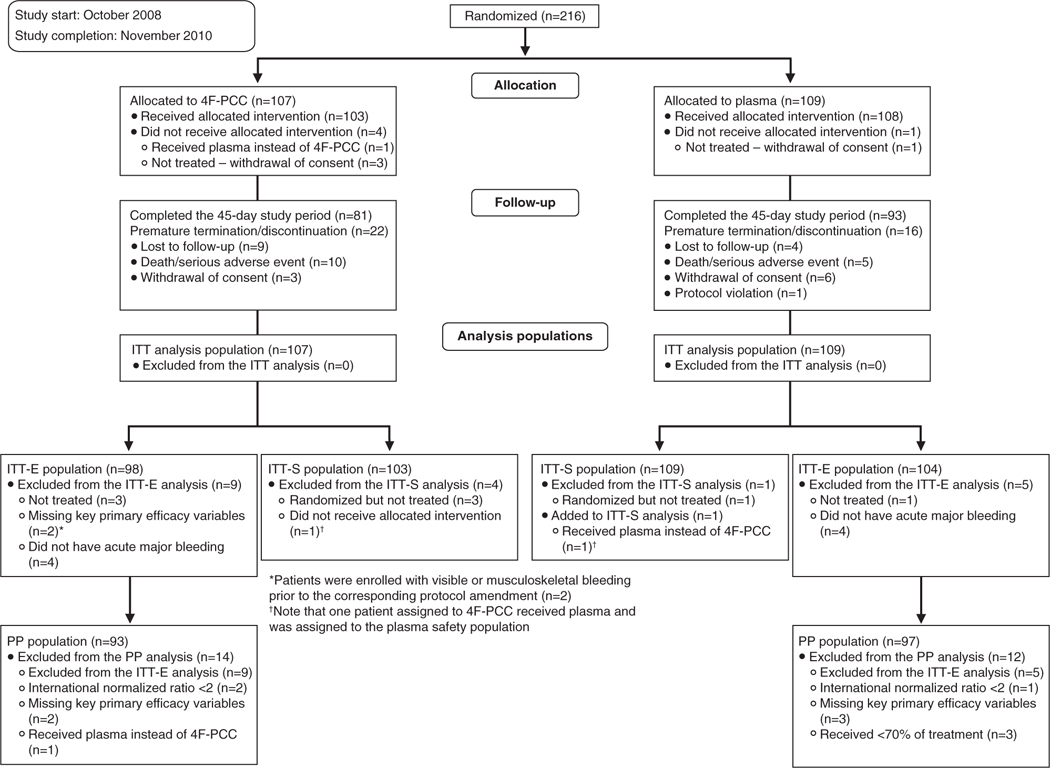
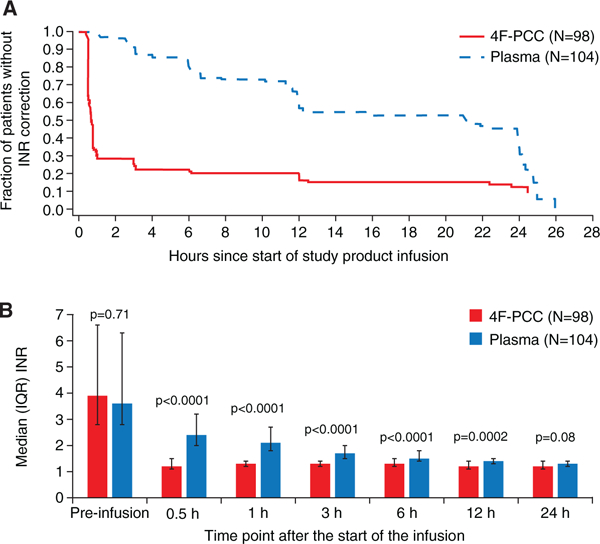
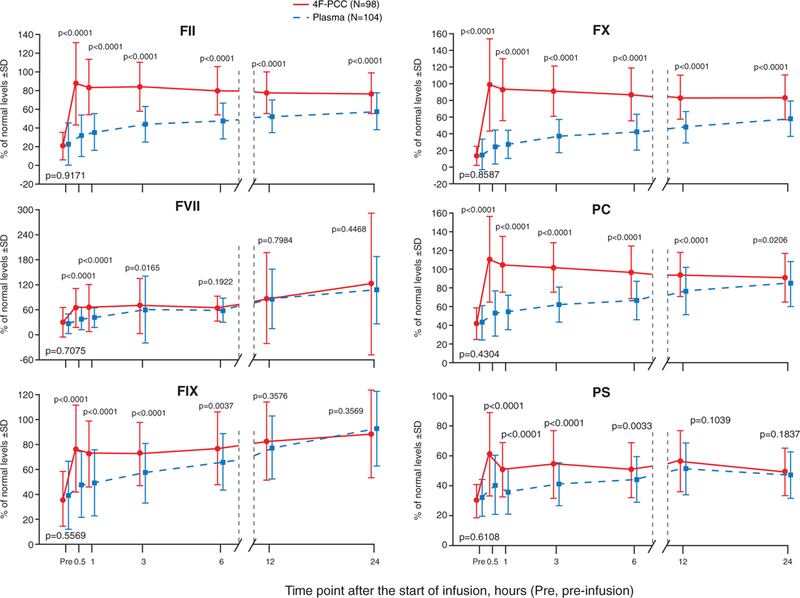
Methods and results: In this phase IIIb, multicenter, open-label, noninferiority trial, nonsurgical patients were randomized to 4F-PCC (containing coagulation factors II, VII, IX, and X and proteins C and S) or plasma. Primary analyses examined whether 4F-PCC was noninferior to plasma for the coprimary end points of 24-hour hemostatic efficacy from start of infusion and international normalized ratio correction (≤1.3) at 0.5 hour after end of infusion. The intention-to-treat efficacy population comprised 202 patients (4F-PCC, n=98; plasma, n=104). Median (range) baseline international normalized ratio was 3.90 (1.8-20.0) for the 4F-PCC group and 3.60 (1.9-38.9) for the plasma group. Effective hemostasis was achieved in 72.4% of patients receiving 4F-PCC versus 65.4% receiving plasma, demonstrating noninferiority (difference, 7.1% [95% confidence interval, -5.8 to 19.9]). Rapid international normalized ratio reduction was achieved in 62.2% of patients receiving 4F-PCC versus 9.6% receiving plasma, demonstrating 4F-PCC superiority (difference, 52.6% [95% confidence interval, 39.4 to 65.9]). Assessed coagulation factors were higher in the 4F-PCC group than in the plasma group from 0.5 to 3 hours after infusion start (P<0.02). The safety profile (adverse events, serious adverse events, thromboembolic events, and deaths) was similar between groups; 66 of 103 (4F-PCC group) and 71 of 109 (plasma group) patients experienced ≥1 adverse event.
Conclusions: 4F-PCC is an effective alternative to plasma for urgent reversal of vitamin K antagonist therapy in major bleeding events, as demonstrated by clinical assessments of bleeding and laboratory measurements of international normalized ratio and factor levels.
Clinical trial registration url: http://www.clinicaltrials.gov. Unique identifier: NCT00708435.
Keywords: anticoagulants; hemorrhage; plasma; prothrombin complex concentrates; vitamin K antagonist.
Conflict of interest statement
Disclosures
Dr Sarode received consulting fees and honoraria from CSL Behring GmbH. Dr Mangione and B. Durn are employees of CSL Behring LLC. Dr Schneider is an employee of CSL Behring GmbH. Dr Goldstein received consulting fees, honoraria, and a research grant from CSL Behring GmbH. Dr Milling received consulting fees from CSL Behring. Dr Refaai reports no conflicts..
Figures
Comment in
-
Four-factor prothrombin complex concentrate for urgent reversal of vitamin K antagonists in patients with major bleeding.Circulation. 2013 Sep 10;128(11):1179-81. doi: 10.1161/CIRCULATIONAHA.113.005107. Epub 2013 Aug 9. Circulation. 2013. PMID: 23935012 No abstract available.
-
ACP Journal Club. 4F-PCC was noninferior to plasma in patients with acute major bleeding who needed urgent VKA reversal.Ann Intern Med. 2014 Apr 15;160(8):JC6. doi: 10.7326/0003-4819-160-8-201404150-02006. Ann Intern Med. 2014. PMID: 24733223 No abstract available.
References
-
- IMS data US National Prescription Audit; MAT (moving annual total) August 2011-July 2012.
-
- Schulman S, Beyth RJ, Kearon C, Levine MN; American College of Chest Physicians. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest. 2008;133(6 suppl):257S–298S. - PubMed
-
- Shehab N, Sperling LS, Kegler SR, Budnitz DS. National estimates of emergency department visits for hemorrhage-related adverse events from clopidogrel plus aspirin and from warfarin. Arch Intern Med. 2010;170:1926–1933. - PubMed
-
- Budnitz D, Lovegrove M, Shehab N, Richards C. Emergency hospitalizations for adverse events in older Americans. N Engl J Med. 2011; 365:2002–2012. - PubMed
-
- Holbrook A, Schulman S, Witt DM, Vandvik PO, Fish J, Kovacs MJ, Svensson PJ, Veenstra DL, Crowther M, Guyatt GH; American College of Chest Physicians. Evidence-based management of anticoagulant therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 suppl):e152S–e184S. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
