

Predicting response to bevacizumab in ovarian cancer: a panel of potential biomarkers informing treatment selection
- PMID: 23935036
- PMCID: PMC3780518
- DOI: 10.1158/1078-0432.CCR-13-0489
Predicting response to bevacizumab in ovarian cancer: a panel of potential biomarkers informing treatment selection
Abstract
Purpose: The aim of this study was to identify and validate novel predictive and/or prognostic serum proteomic biomarkers in patients with epithelial ovarian cancer (EOC) treated as part of the phase III international ICON7 clinical trial.
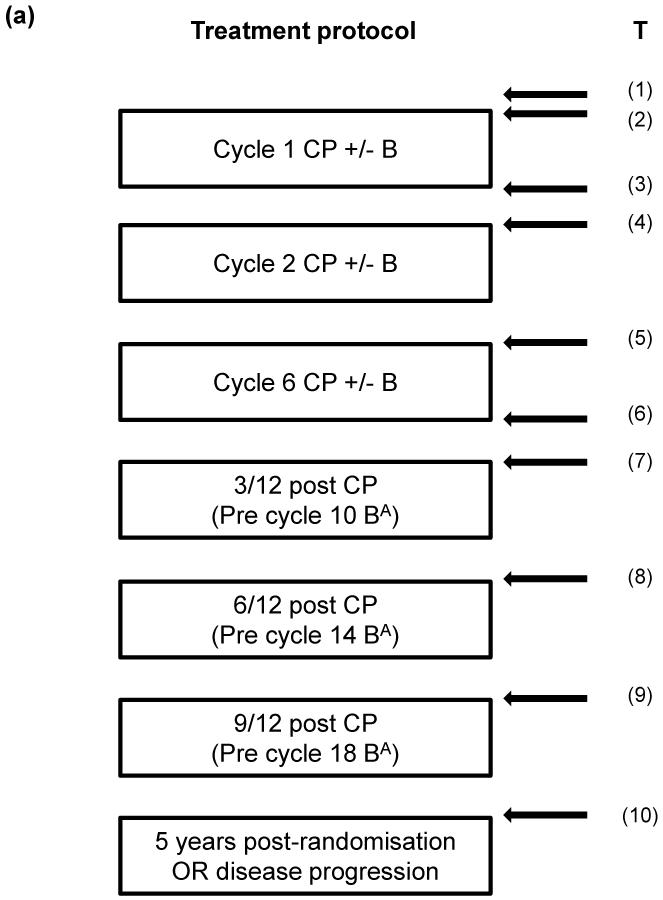
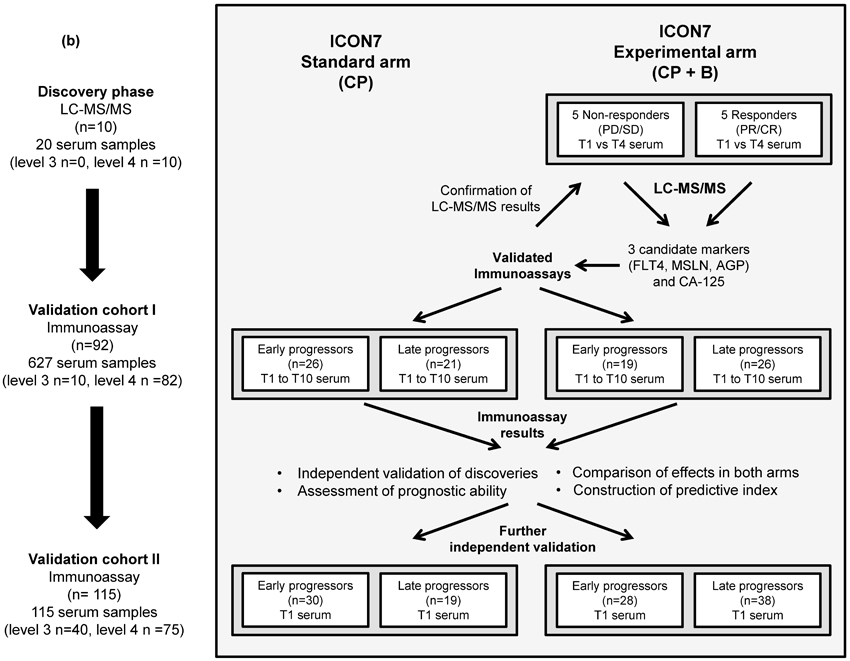
Experimental design: ICON7 was a phase III international trial in EOC which showed a modest but statistically significant benefit in progression-free survival (PFS) with the addition of bevacizumab to standard chemotherapy. Serum samples from 10 patients who received bevacizumab (five responders and five nonresponders) were analyzed by mass spectrometry to identify candidate biomarkers. Initial validation and exploration by immunoassay was undertaken in an independent cohort of 92 patients, followed by a second independent cohort of 115 patients (taken from across both arms of the trial).
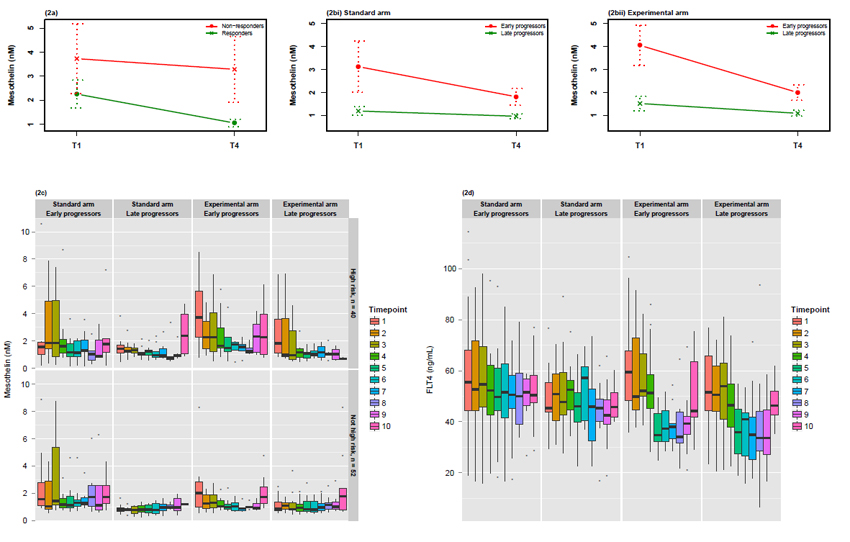
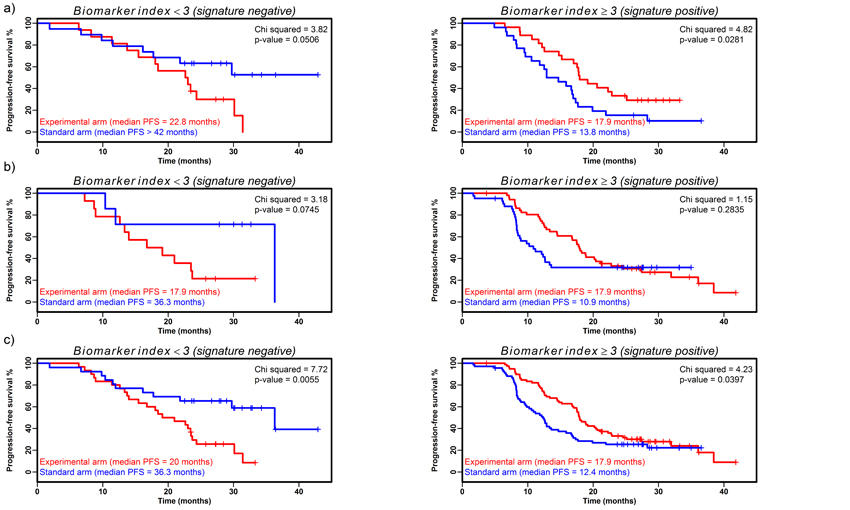
Results: Three candidate biomarkers were identified: mesothelin, fms-like tyrosine kinase-4 (FLT4), and α1-acid glycoprotein (AGP). Each showed evidence of independent prognostic potential when adjusting for high-risk status in initial (P < 0.02) and combined (P < 0.01) validation cohorts. In cohort I, individual biomarkers were not predictive of bevacizumab benefit; however, when combined with CA-125, a signature was developed that was predictive of bevacizumab response and discriminated benefit attributable to bevacizumab better than clinical characteristics. The signature showed weaker evidence of predictive ability in validation cohort II, but was still strongly predictive considering all samples (P = 0.001), with an improvement in median PFS of 5.5 months in signature-positive patients in the experimental arm compared with standard arm.
Conclusions: This study shows a discriminatory signature comprising mesothelin, FLT4, AGP, and CA-125 as potentially identifying those patients with EOC more likely to benefit from bevacizumab. These results require validation in further patient cohorts.
©2013 AACR.
Figures
Comment in
-
Biomarkers and response to bevacizumab--letter.Clin Cancer Res. 2014 Feb 15;20(4):1056-7. doi: 10.1158/1078-0432.CCR-13-2763. Clin Cancer Res. 2014. PMID: 24536076 No abstract available.
-
Biomarkers and response to bevacizumab--response.Clin Cancer Res. 2014 Feb 15;20(4):1058. doi: 10.1158/1078-0432.CCR-13-3269. Clin Cancer Res. 2014. PMID: 24536077 No abstract available.
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Stuart GC, Kitchener H, Bacon M, duBois A, Friedlander M, Ledermann J, et al. 2010 Gynecologic Cancer InterGroup (GCIG) consensus statement on clinical trials in ovarian cancer: report from the Fourth Ovarian Cancer Consensus Conference. Int J Gynecol Cancer. 2011;21:750–5. - PubMed
-
- Perren TJ, Swart AM, Pfisterer J, Ledermann JA, Pujade-Lauraine E, Kristensen G, et al. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. 2011;365:2484–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
