

Diagnostic value of dynamics serum sCD163, sTREM-1, PCT, and CRP in differentiating sepsis, severity assessment, and prognostic prediction
- PMID: 23935252
- PMCID: PMC3713373
- DOI: 10.1155/2013/969875
Diagnostic value of dynamics serum sCD163, sTREM-1, PCT, and CRP in differentiating sepsis, severity assessment, and prognostic prediction
Abstract
Objective: To describe the dynamics changes of sCD163, soluble serum triggering receptor expressed on myeloid cells-1 (sTREM-1), procalcitonin (PCT), and C-reactive protein (CRP) during the course of sepsis, as well as their outcome prediction.
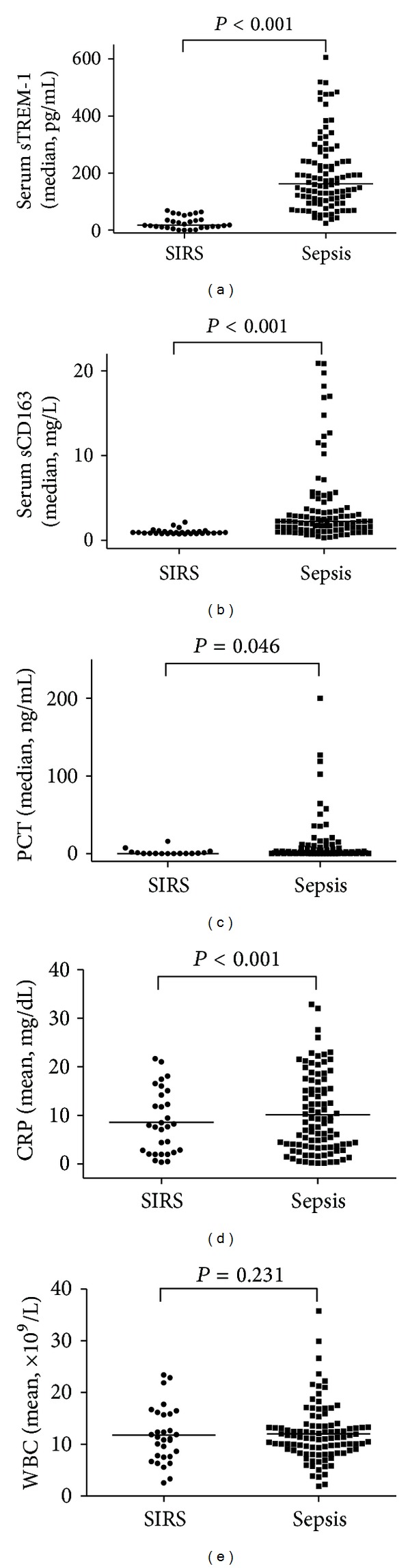
Patients and methods: An SIRS group (30 cases) and a sepsis group (100 cases) were involved in this study. Based on a 28-day survival, the sepsis was further divided into the survivors' and nonsurvivors' groups. Serum sTREM-1, sCD163, PCT, CRP, and WBC counts were tested on days 1, 3, 5, 7, 10, and 14.
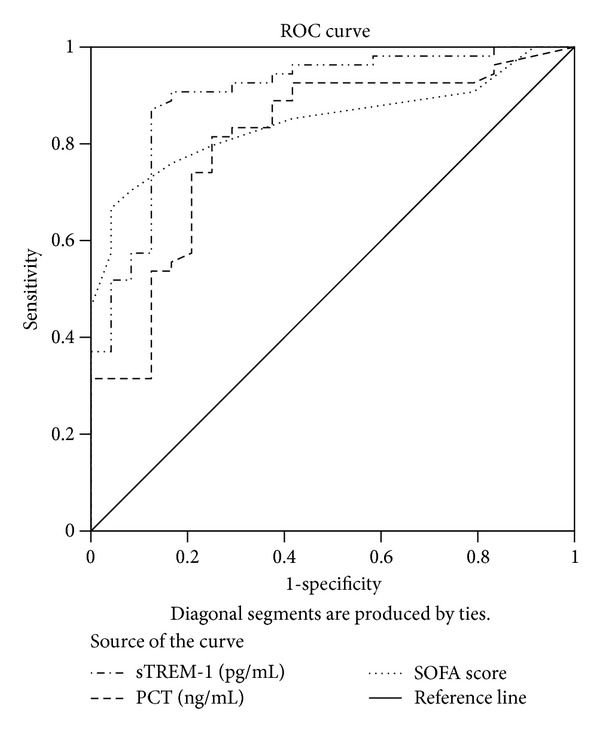
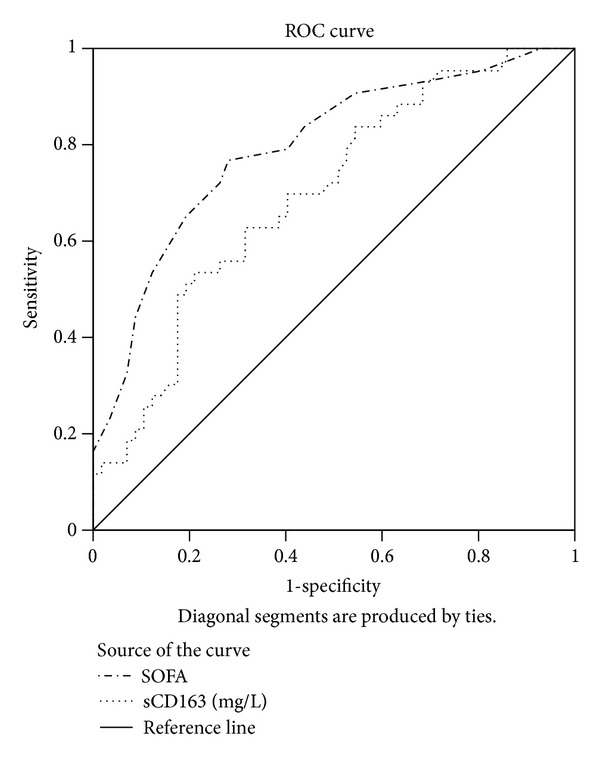
Results: On the ICU admission, the sepsis group displayed higher levels of sTREM-1, sCD163, PCT, and CRP than the SIRS group (P < 0.05). Although PCT and sTREM-1 are good markers to identify severity, sTREM-1 is more reliable, which proved to be a risk factor related to sepsis. During a 14-day observation, sCD163, sTREM-1, PCT, and SOFA scores continued to climb among nonsurvivors, while their WBC and CRP went down. Both sCD163 and SOFA scores are risk factors impacting the survival time.
Conclusion: With regard to sepsis diagnosis and severity, sTREM-1 is more ideal and constitutes a risk factor. sCD163 is of a positive value in dynamic prognostic assessment and may be taken as a survival-impacting risk factor.
Figures


References
-
- Kochanek KD, Murphy SL, Anderson RN, Scott C. Deaths: final data for 2002. National Vital Statistics Reports. 2004;53(5):1–115. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. The New England Journal of Medicine. 2003;348(16):1546–1554. - PubMed
-
- Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. The New England Journal of Medicine. 2003;348(2):138–150. - PubMed
-
- Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Critical Care Medicine. 2004;32(3):858–873. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
