

Reduced heart rate variability in social anxiety disorder: associations with gender and symptom severity
- PMID: 23936207
- PMCID: PMC3728204
- DOI: 10.1371/journal.pone.0070468
Reduced heart rate variability in social anxiety disorder: associations with gender and symptom severity
Abstract
Background: Polyvagal theory emphasizes that autonomic nervous system functioning plays a key role in social behavior and emotion. The theory predicts that psychiatric disorders of social dysfunction are associated with reduced heart rate variability, an index of autonomic control, as well as social inhibition and avoidance. The purpose of this study was to examine whether heart rate variability was reduced in treatment-seeking patients diagnosed with social anxiety disorder, a disorder characterized by social fear and avoidance.
Methods: Social anxiety patients (n = 53) were recruited prior to receiving psychological therapy. Healthy volunteers were recruited through the University of Sydney and the general community and were matched by gender and age (n = 53). Heart rate variability was assessed during a five-minute recording at rest, with participants completing a range of self-report clinical symptom measures.
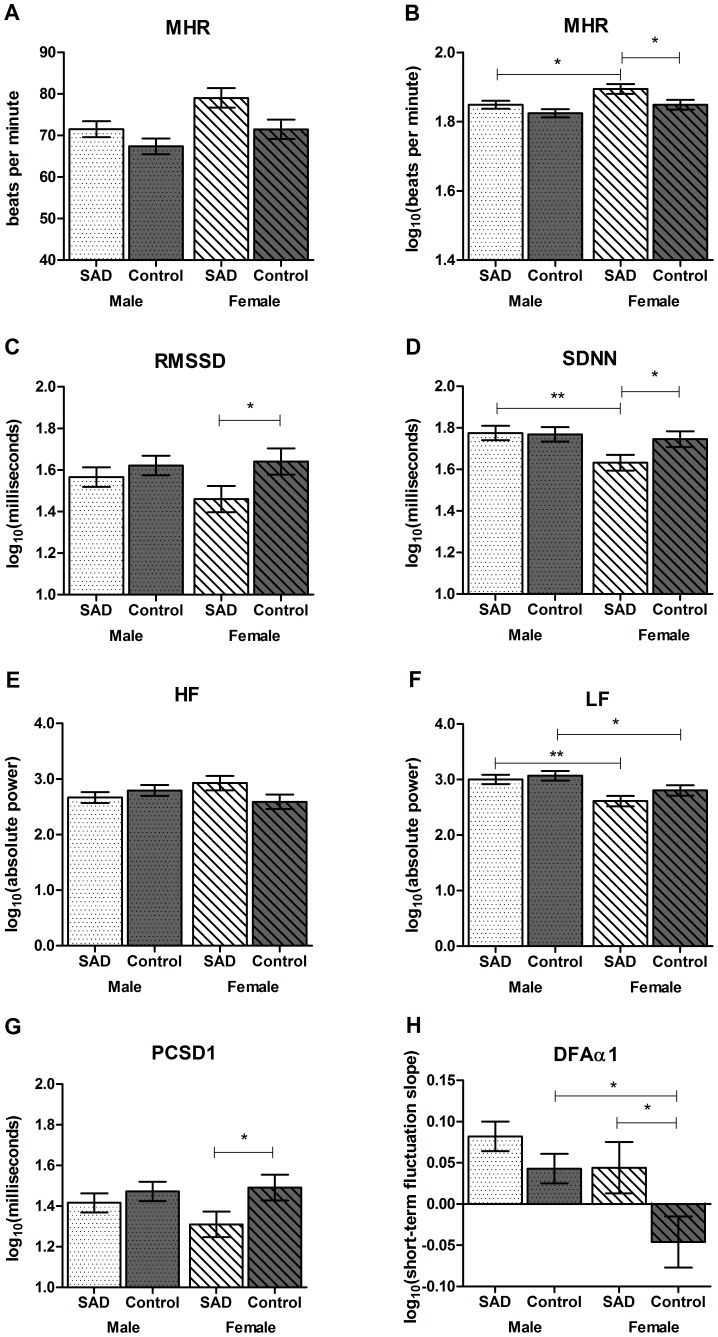
Results: Compared to controls, participants with social anxiety exhibited significant reductions across a number of heart rate variability measures. Reductions in heart rate variability were observed in females with social anxiety, compared to female controls, and in patients taking psychotropic medication compared to non-medicated patients. Finally, within the clinical group, we observed significant associations between reduced heart rate variability and increased social interaction anxiety, psychological distress, and harmful alcohol use.
Conclusions: The results of this study confirm that social anxiety disorder is associated with reduced heart rate variability. Resting state heart rate variability may therefore be considered a marker for social approach-related motivation and capacity for social engagement. Additionally, heart rate variability may provide a useful biomarker to explain underlying difficulties with social approach, impaired stress regulation, and behavioral inhibition, especially in disorders associated with significant impairments in these domains.
Conflict of interest statement
Figures
References
-
- Kawachi I, Sparrow D, Vokonas P, Weiss S (1994) Symptoms of anxiety and risk of coronary heart disease. The Normative Aging Study. Circulation 90: 2225–2229. - PubMed
-
- Friedman B (2007) An autonomic flexibility–neurovisceral integration model of anxiety and cardiac vagal tone. Biological Psychology 74: 185–199. - PubMed
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas K, et al. (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry 62: 593–602. - PubMed
-
- Clark DM, Wells A (1995) A cognitive model of social phobia. In: Heimberg R, Liebowitz M, Hope DA, Schneier FR, editors. Social phobia: Diagnosis, assessment and treatment. New York: Guilford Press. 69–93.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
