

Relevance of distinct monocyte subsets to clinical course of ischemic stroke patients
- PMID: 23936327
- PMCID: PMC3732285
- DOI: 10.1371/journal.pone.0069409
Relevance of distinct monocyte subsets to clinical course of ischemic stroke patients
Abstract
Background and purpose: The most common strategy for treating patients with acute ischemic stroke is thrombolytic therapy, though only a few patients receive benefits because of the narrow time window. Inflammation occurring in the central nervous system (CNS) in association with ischemia is caused by immune cells including monocytes and involved in lesion expansion. If the specific roles of monocyte subsets in stroke can be revealed, they may become an effective target for new treatment strategies.
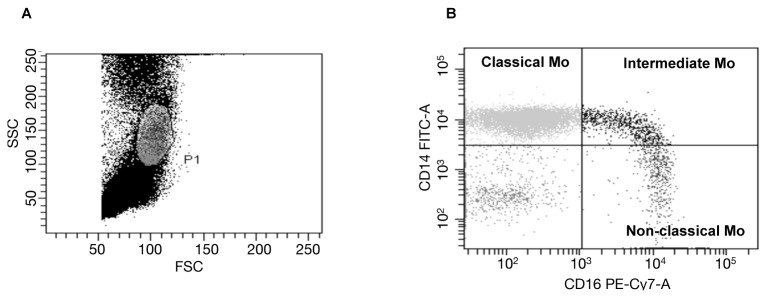
Methods: We performed immunological examinations of 36 consecutive ischemic stroke patients within 2 days of onset and compared the results with 24 age-matched patients with degenerative disorders. The stroke patients were repeatedly tested for the proportions of monocyte subsets in blood, and serum levels of pro- and anti-inflammatory cytokines immediately after admission, on days 3-7 and 12-16 after stroke onset, and on the day of discharge. In addition, immunological measurements were analyzed for relationships to stroke subtypes and complications, including progressive infarction (PI) and stroke-associated infection (SAI).
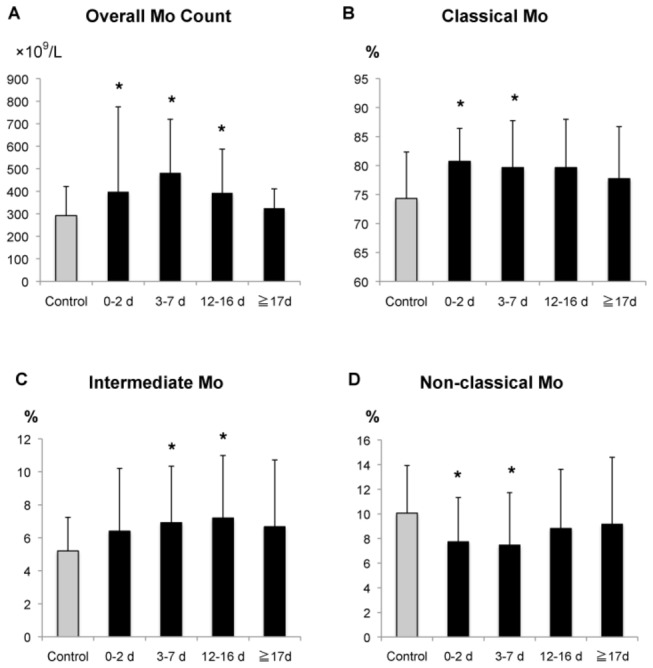
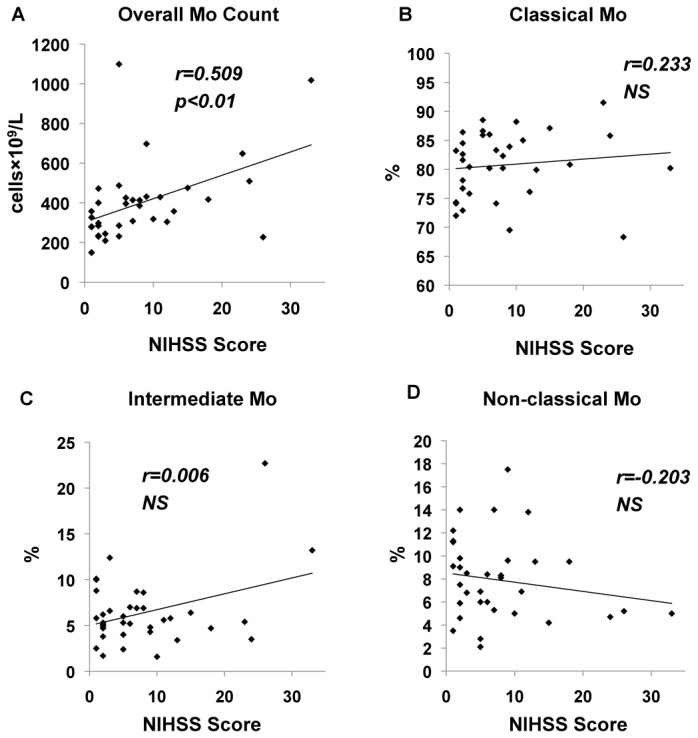
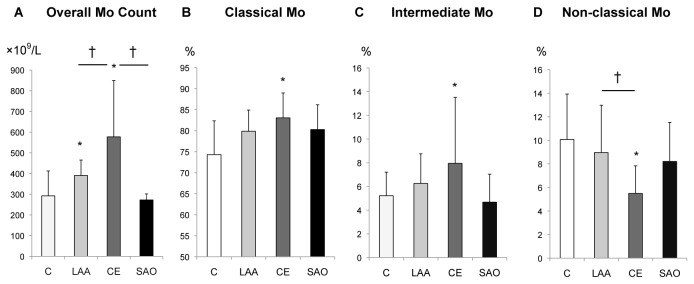
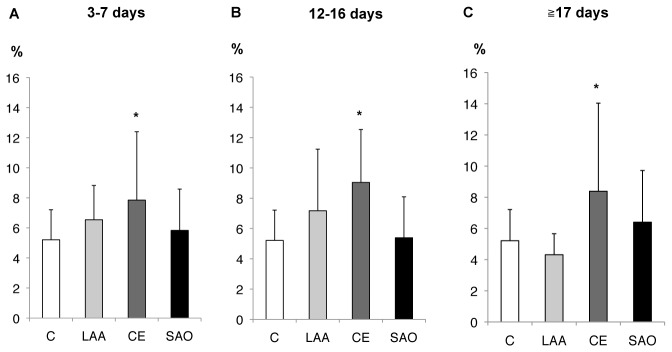
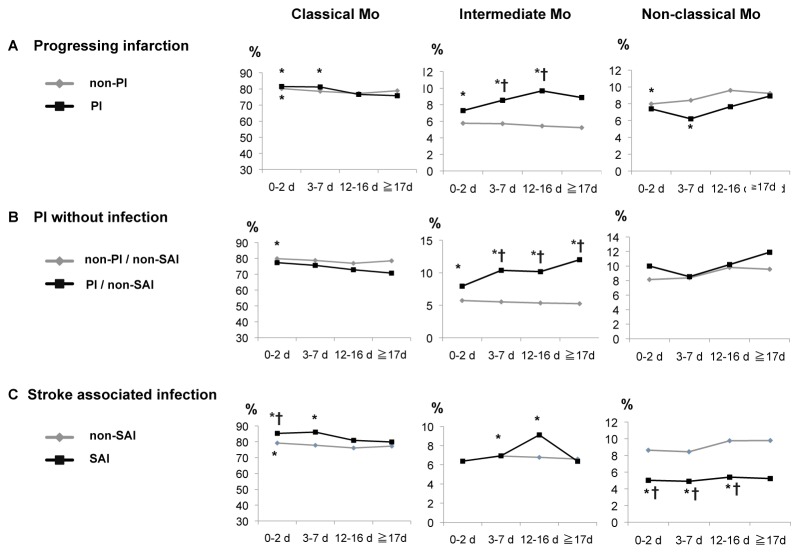
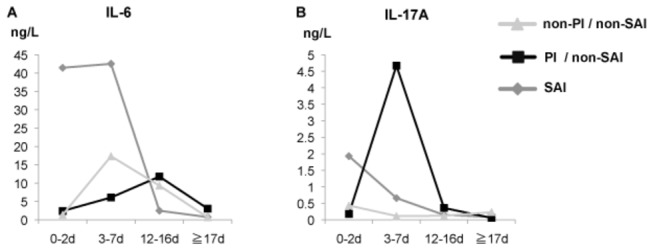
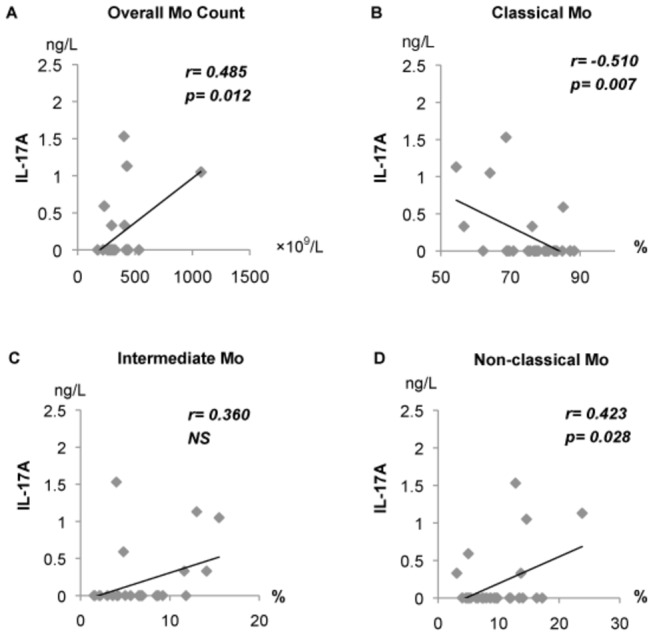
Results: Monocyte count was significantly increased from 0-16 days after stroke as compared to the controls (p<0.05). CD14(high)CD16(-) classical and CD14(high)CD16(+) intermediate monocytes were significantly increased from 0-7 and 3-16 days after stroke, respectively (p<0.05), whereas CD14 (dim)CD16(high) non-classical monocytes were decreased from 0-7 days (p<0.05). Cardioembolic infarction was associated with a persistent increase in intermediate monocytes. Furthermore, intermediate monocytes were significantly increased in patients with PI (p<0.05), while non-classical monocytes were decreased in those with SAI (p<0.05). IL-17A levels were positively correlated with monocyte count (r=0.485, p=0.012) as well as the percentage of non-classical monocytes (r=0.423, p=0.028), and negatively with that of classical monocytes (r=-0.51, p=0.007) during days 12-16.
Conclusions: Our findings suggest that CD14(high)CD16(+) intermediate monocytes have a role in CNS tissue damage during acute and subacute phases in ischemic stroke especially in relation to cardioembolism.
Conflict of interest statement
Figures
References
-
- Moskowitz MA, Lo EH, Iadecola C (2010) The science of stroke: mechanisms in search of treatments. Neuron 67: 181-198. doi:10.1016/j.neuron.2010.07.002. PubMed: 20670828. - DOI - PMC - PubMed
-
- Iadecola C, Anrather J (2011) The immunology of stroke: from mechanisms to translation. Nat Med 17: 796-808. doi:10.1038/nm.2399. PubMed: 21738161. - DOI - PMC - PubMed
-
- Tuttolomondo A, Di Raimondo D, di Sciacca R, Pinto A, Licata G (2008) Inflammatory cytokines in acute ischemic stroke. Curr Pharm Des 14: 3574-3589. doi:10.2174/138161208786848739. PubMed: 19075734. - DOI - PubMed
-
- Castellanos M, Castillo J, García MM, Leira R, Serena J et al. (2002) Inflammation-mediated damage in progressing lacunar infarctions: a potential therapeutic target. Stroke 33: 982-987. doi:10.1161/hs0402.105339. PubMed: 11935048. - DOI - PubMed
-
- Yan J, Greer JM, McCombe PA (2012) Prolonged elevation of cytokine levels after human acute ischaemic stroke with evidence of individual variability. J Neuroimmunol 246: 78-84. doi:10.1016/j.jneuroim.2012.02.013. PubMed: 22425021. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
