

Bronchiectasis-associated hospitalizations in Germany, 2005-2011: a population-based study of disease burden and trends
- PMID: 23936489
- PMCID: PMC3731262
- DOI: 10.1371/journal.pone.0071109
Bronchiectasis-associated hospitalizations in Germany, 2005-2011: a population-based study of disease burden and trends
Abstract
Background: Representative population-based data on the epidemiology of bronchiectasis in Europe are limited. The aim of the present study was to investigate the current burden and the trends of bronchiectasis-associated hospitalizations and associated conditions in Germany in order to inform focused patient care and to facilitate the allocation of healthcare resources.
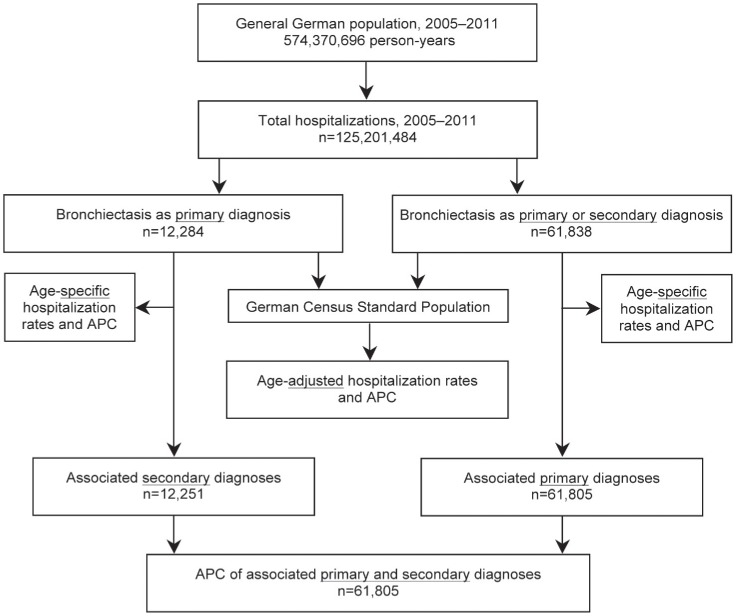
Methods: The nationwide diagnosis-related groups hospital statistics for the years 2005-2011 were used in order to identify hospitalizations with bronchiectasis as any hospital discharge diagnosis according to the International Classification of Diseases, 10th revision, code J47, (acquired) bronchiectasis. Poisson log-linear regression analysis was used to assess the significance of trends. In addition, the overall length of hospital stay (LOS) and the in-hospital mortality in comparison to the nationwide overall mortality due to bronchiectasis as the primary diagnosis was assessed.
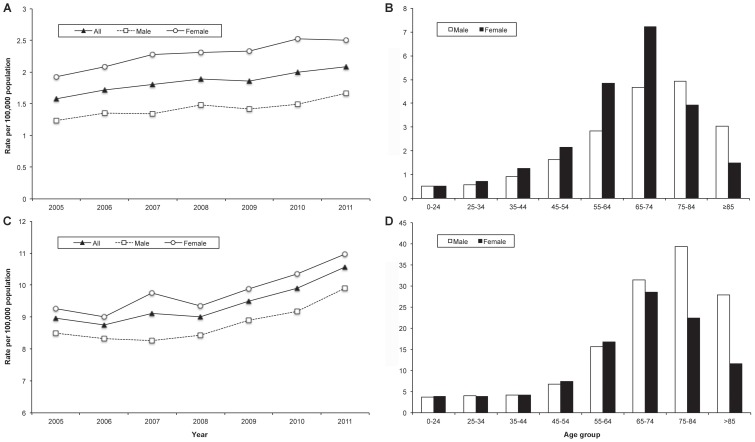
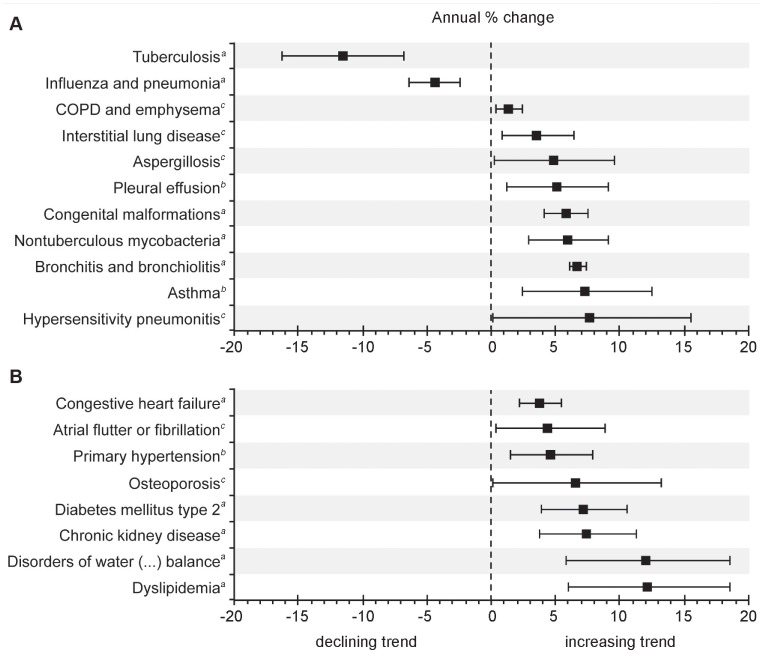
Results: Overall, 61,838 records with bronchiectasis were extracted from more than 125 million hospitalizations. The average annual age-adjusted rate for bronchiectasis as any diagnosis was 9.4 hospitalizations per 100,000 population. Hospitalization rates increased significantly during the study period, with the highest rate of 39.4 hospitalizations per 100,000 population among men aged 75-84 years and the most pronounced average annual increases among females. Besides numerous bronchiectasis-associated conditions, chronic obstructive pulmonary disease (COPD) was most frequently found in up to 39.2% of hospitalizations with bronchiectasis as the primary diagnosis. The mean LOS was comparable to that for COPD. Overall, only 40% of bronchiectasis-associated deaths occurred inside the hospital.
Conclusions: The present study provides evidence of a changing epidemiology and a steadily increasing prevalence of bronchiectasis-associated hospitalizations. Moreover, it confirms the diversity of bronchiectasis-associated conditions and the possible association between bronchiectasis and COPD. As the major burden of disease may be managed out-of-hospital, prospective patient registries are needed to establish the exact prevalence of bronchiectasis according to the specific underlying condition.
Conflict of interest statement
Figures
References
-
- Saynajakangas O, Keistinen T, Tuuponen T, Kivela SL (1997) Bronchiectasis in Finland: trends in hospital treatment. Respir Med 91: 395–398. - PubMed
-
- Tsang KW, Tipoe GL (2004) Bronchiectasis: not an orphan disease in the East. Int J Tuberc Lung Dis 8: 691–702. - PubMed
-
- Weycker D, Edelsberg J, Oster G, Tino G (2005) Prevalence and economic burden of bronchiectasis. Clin Pulm Med 12: 205–209.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
