

Surgical treatment of large substernal thyroid goiter: analysis of 12 patients
- PMID: 23936586
- PMCID: PMC3731179
Surgical treatment of large substernal thyroid goiter: analysis of 12 patients
Abstract
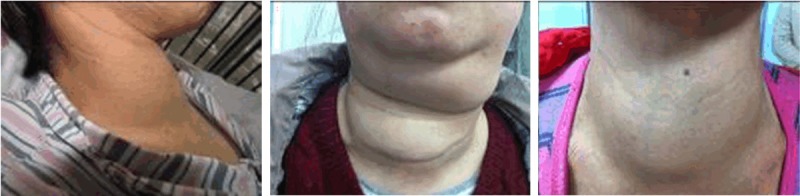
This study was carried out to evaluate the clinical presentation, surgical treatment, complications, and risk of malignancy for large substernal goiter. From March 2010 to December 2012, 12 patients with large substernal thyroid goiter who underwent surgery in our Department were enrolled in the study. Their medical records were retrospectively analyzed. Collar-shaped incision was adequate for resection of the lesions in 10 (83%) patients, while two (17%) patients required combined cervical-thoracic incision. In addition, one case was subjected to postoperative tracheotomy. Transient hypocalcaemia occurred in one case. The incidence of transient hoarseness, tracheomalacia and hypothyroidism was 8.3%. There was no perioperative bleeding, thyroid storm as well as other serious complications. All patients were clinically cured. Therefore, cervical collar incision is nearly always adequate for most cases of larger substernal goiter, and sternotomy can be avoided. Furthermore, the application of intraoperative ultrasonic knife can effectively reduce intraoperative and postoperative complications. Aggressive perioperative management is crucial for the successful removal of large substernal goiter.
Keywords: Substernal goiter; complications; operative approach; ultrasonic knife.
Figures






References
-
- Parra-Membrives P, Sánchez-Blanco JM, Gómez-Rubio D, Recio-Moyano G, Diaz-Roldán J. Retrosternal goiters: safety of surgical treatment. Int Surg. 2003;88:205–210. - PubMed
-
- Foroulis CN, Rammos KS, Sileli MN, Papakonstantinou C. Primary intrathoracic goiter: a rare and potentially serious entity. Thyroid. 2009;19:213–218. - PubMed
-
- Batori M, Chatelou E, Straniero A, Mariotta G, Palombi L, Pastore P, Casella G, Casella MC. Substernal goiters. Eur Rev Med Pharmacol Sci. 2005;9:355–359. - PubMed
-
- Kilic D, Findikcioglu A, Ekici Y, Alemdaroglu U, Hekimoglu K, Hatipoglu A. When is transthoracic approach indicated in retrosternal goiters? Ann Thorac Cardiovasc Surg. 2011;17:250–253. - PubMed
-
- White ML, Doherty GM, Gauger PG. Evidence-based surgical management of substernal goiter. World J Surg. 2008;32:1285–1300. - PubMed
LinkOut - more resources
Full Text Sources