

Diffusion-weighted MRI as a biomarker for treatment response in glioma
- PMID: 23936625
- PMCID: PMC3734866
- DOI: 10.2217/cns.12.25
Diffusion-weighted MRI as a biomarker for treatment response in glioma
Abstract
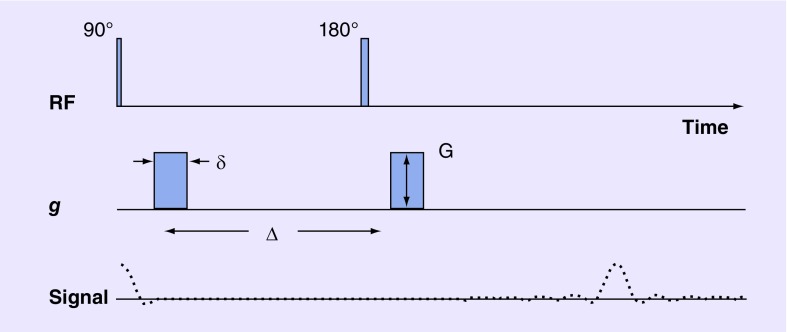
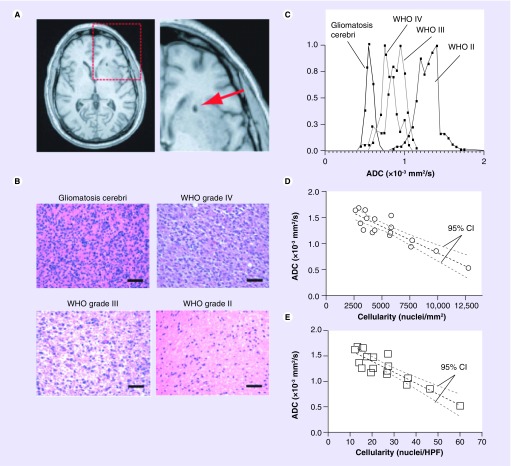
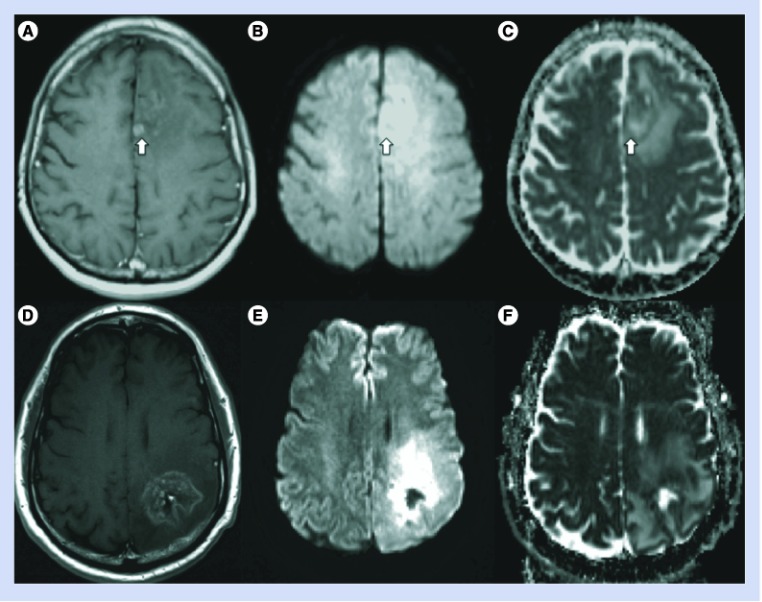
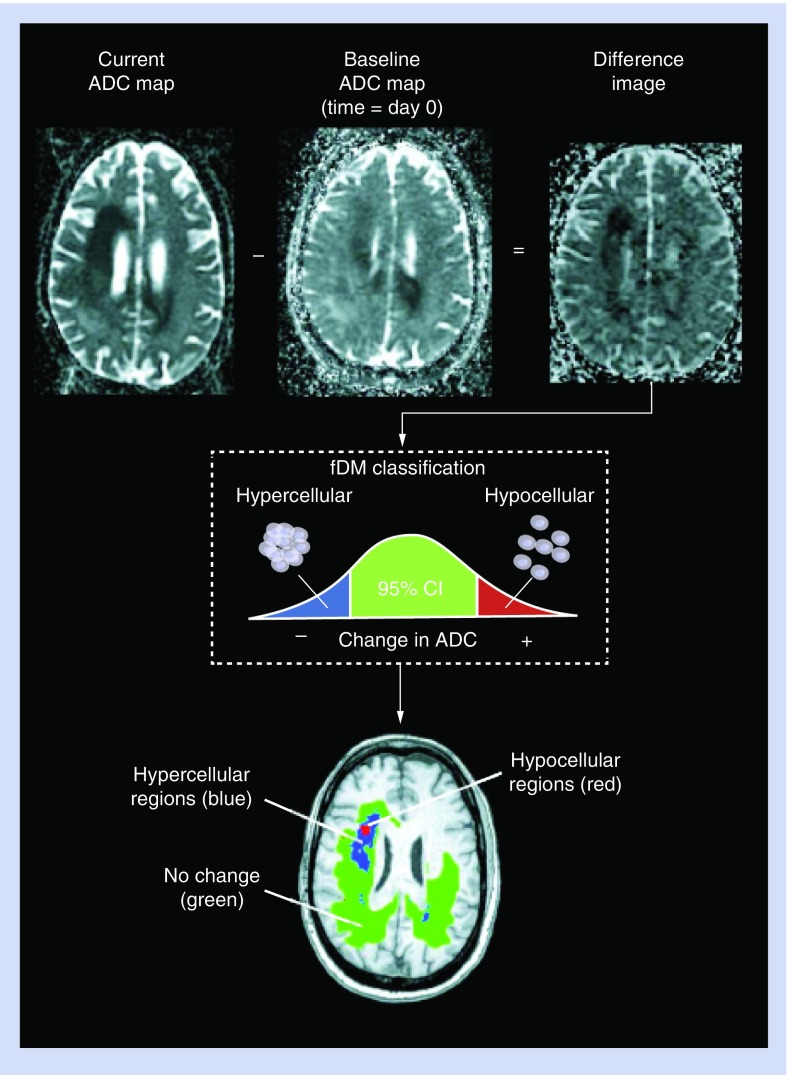
Diffusion-weighted imaging (DWI) is a powerful MRI method, which probes abnormalities of tissue structure by detecting microscopic changes in water mobility at a cellular level beyond what is available with other imaging techniques. Accordingly, DWI has the potential to identify pathology before gross anatomic changes are evident on standard anatomical brain images. These features of tissue characterization and earlier detection are what make DWI particularly appealing for the evaluation of gliomas and the newer therapies where standard anatomical imaging is proving insufficient. This article focuses on the basic principles and applications of DWI, and its derived parameter, the apparent diffusion coefficient, for the purposes of diagnosis and evaluation of glioma, especially in the context of monitoring response to therapy.
Conflict of interest statement
Figures
References
-
- MacDonald DR, Cascino TL, Schold SC, Cairncross JG. Response criteria for Phase II studies of malignant glioma. J. Clin. Oncol. 1990;8:1277–1280. - PubMed
-
- Brandsma D, van den Bent MJ. Pseudoprogression and pseudoresponse in the treatment of gliomas. Curr. Opin Neurol. 2009;22:633–638. - PubMed
-
- MacDonald DR, Cascino TL, Schold SC, Calmcross JG. Response criteria for Phase II studies of supratentorial malignant glioma. J. Clin. Oncol. 1990;8(7):1277–1280. - PubMed
-
- Wen PY, MacDonald DR, Reardon DA, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J. Clin. Oncol. 2010;28(11):1963–1972. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical