

The Correlation between Chronic Periodontitis and Oral Cancer
- PMID: 23936684
- PMCID: PMC3725788
- DOI: 10.1155/2013/262410
The Correlation between Chronic Periodontitis and Oral Cancer
Abstract
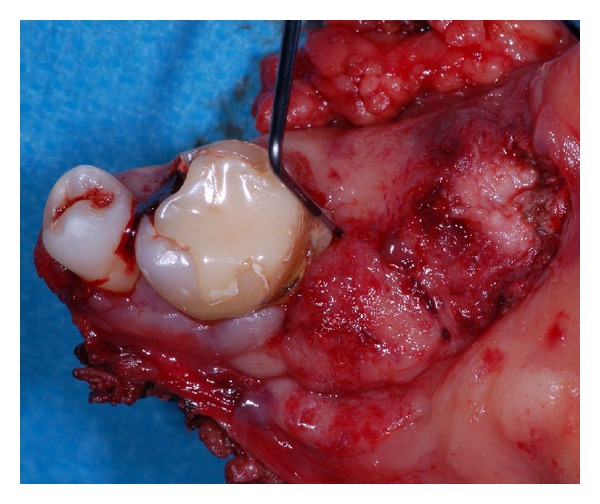
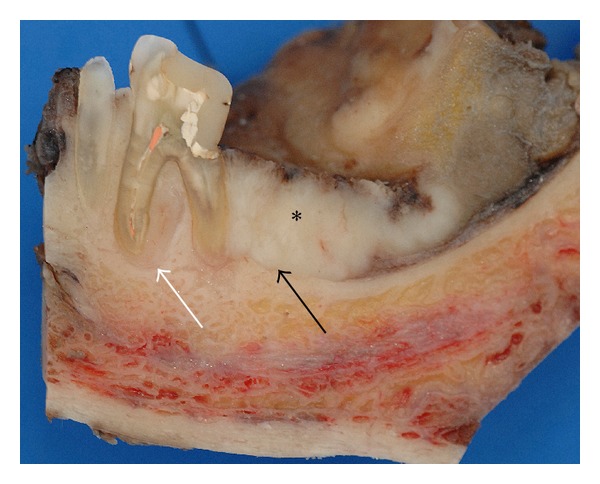
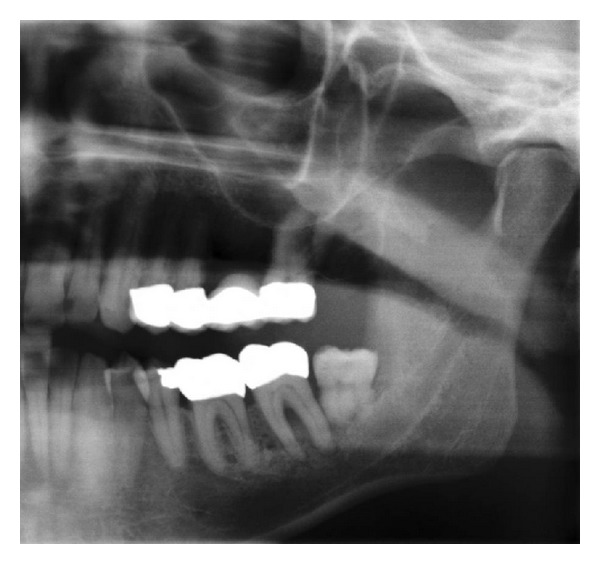
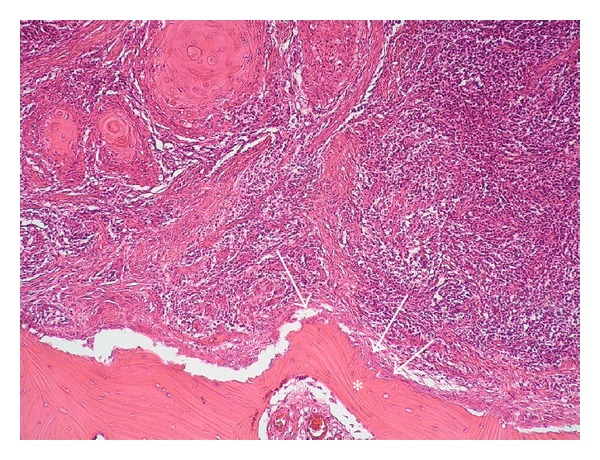
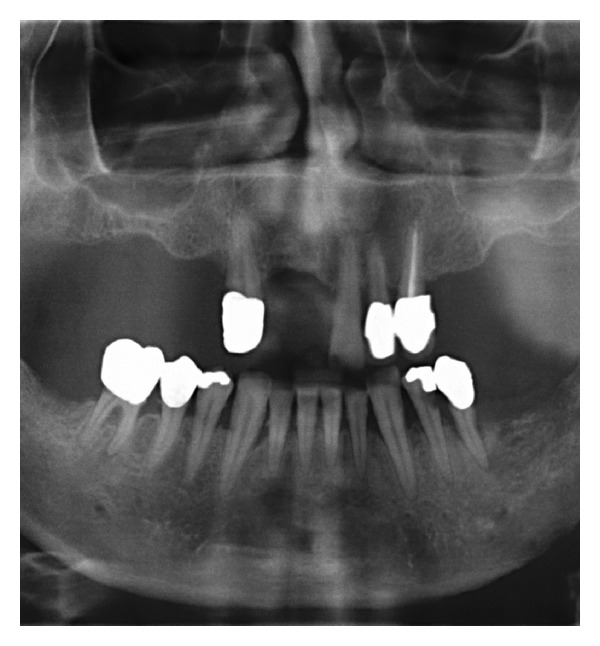
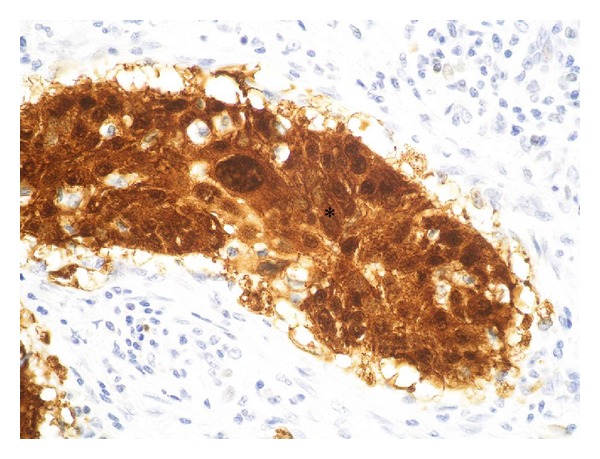
Infections are increasingly considered as potential trigger for carcinogenesis apart from risk factors like alcohol and tobacco. The discussion about human papilloma virus (HPV) in oral squamous cell carcinoma (OSCC) points at a general role of infection for the development of oral carcinomas. Furthermore, first studies describe a correlation between chronic periodontitis and OSCC, thus, characterizing chronic inflammation as being a possible trigger for OSCC. In front of this background, we present four well-documented clinical cases. All patients showed a significant anatomical relation between OSCC and clinical signs of chronic periodontitis. The interindividual differences of the clinical findings lead to different theoretical concepts: two with coincidental appearance of OSCC and chronic periodontitis and two with possible de novo development of OSCC triggered by chronic inflammation. We conclude that the activation of different inflammatory cascades by chronic periodontitis negatively affects mucosa and bone. Furthermore, the inflammatory response has the potential to activate carcinogenesis. Apart from a mere coincidental occurrence, two out of four patients give first clinical hints for a model wherein chronic periodontitis represents a potential risk factor for the development of OSCC.
Figures








References
-
- Landis SH, Murray T, Bolden S, Wingo PA. Cancer Statistics, 1999. CA: A Cancer Journal for Clinicians. 1999;49(1):8–31. - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA: A Cancer Journal for Clinicians. 2005;55(2):74–108. - PubMed
-
- Rusin P, Markiewicz L, Majsterek I. Genetic predeterminations of head and neck cancer. Postępy Higieny i Medycyny Doświadczalnej. 2008;62:490–501. - PubMed
-
- Rödström P-O, Jontell M, Mattsson U, Holmberg E. Cancer and oral lichen planus in a Swedish population. Oral Oncology. 2004;40(2):131–138. - PubMed
-
- Pelucchi C, Gallus S, Garavello W, Bosetti C, Vecchia CL. Alcohol and tobacco use, and cancer risk for upper aerodigestive tract and liver. European Journal of Cancer Prevention. 2008;17(4):340–344. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
