

Trends and outcomes in the use of surgery and radiation for the treatment of locally advanced esophageal cancer: a propensity score adjusted analysis of the surveillance, epidemiology, and end results registry from 1998 to 2008
- PMID: 23937253
- PMCID: PMC3923844
- DOI: 10.1111/dote.12123
Trends and outcomes in the use of surgery and radiation for the treatment of locally advanced esophageal cancer: a propensity score adjusted analysis of the surveillance, epidemiology, and end results registry from 1998 to 2008
Abstract
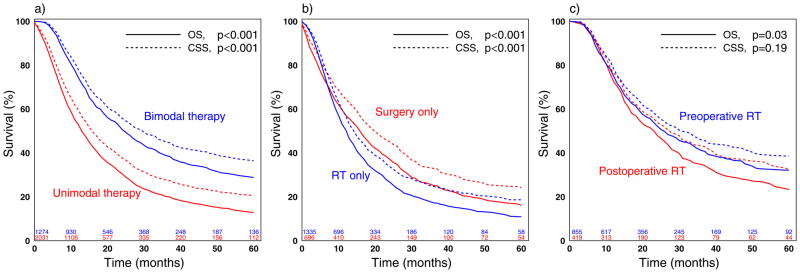
We examined outcomes and trends in surgery and radiation use for patients with locally advanced esophageal cancer, for whom optimal treatment isn't clear. Trends in surgery and radiation for patients with T1-T3N1M0 squamous cell or adenocarcinoma of the mid or distal esophagus in the Surveillance, Epidemiology, and End Results database from 1998 to 2008 were analyzed using generalized linear models including year as predictor; Surveillance, Epidemiology, and End Results doesn't record chemotherapy data. Local treatment was unimodal if patients had only surgery or radiation and bimodal if they had both. Five-year cancer-specific survival (CSS) and overall survival (OS) were analyzed using propensity-score adjusted Cox proportional-hazard models. Overall 5-year survival for the 3295 patients identified (mean age 65.1 years, standard deviation 11.0) was 18.9% (95% confidence interval: 17.3-20.7). Local treatment was bimodal for 1274 (38.7%) and unimodal for 2021 (61.3%) patients; 1325 (40.2%) had radiation alone and 696 (21.1%) underwent only surgery. The use of bimodal therapy (32.8-42.5%, P = 0.01) and radiation alone (29.3-44.5%, P < 0.001) increased significantly from 1998 to 2008. Bimodal therapy predicted improved CSS (hazard ratios [HR]: 0.68, P < 0.001) and OS (HR: 0.58, P < 0.001) compared with unimodal therapy. For the first 7 months (before survival curve crossing), CSS after radiation therapy alone was similar to surgery alone (HR: 0.86, P = 0.12) while OS was worse for surgery only (HR: 0.70, P = 0.001). However, worse CSS (HR: 1.43, P < 0.001) and OS (HR: 1.46, P < 0.001) after that initial timeframe were found for radiation therapy only. The use of radiation to treat locally advanced mid and distal esophageal cancers increased from 1998 to 2008. Survival was best when both surgery and radiation were used.
Keywords: esophageal cancer; esophagectomy; radiation therapy; surgery.
© 2013 Wiley Periodicals, Inc. and the International Society for Diseases of the Esophagus.
Conflict of interest statement
The authors have no other potential conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript.
Figures
References
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349:2241–52. - PubMed
-
- Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Waldron W, et al. SEER Cancer Statistics Review, 1975–2008. National Cancer Institute; Bethesda, MD: 2011. http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the SEER web site, 2011.
-
- Paulson EC, Ra J, Armstrong K, Wirtalla C, Spitz F, Kelz RR. Underuse of esophagectomy as treatment for resectable esophageal cancer. Arch Surg. 2008;143:1198–203. discussion 203. - PubMed
-
- Dubecz A, Sepesi B, Salvador R, Polomsky M, Watson TJ, Raymond DP, et al. Surgical resection for locoregional esophageal cancer is underutilized in the United States. J Am Coll Surg. 2010;211:754–61. - PubMed
-
- Bedenne L, Michel P, Bouche O, Milan C, Mariette C, Conroy T, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol. 2007;25:1160–8. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
