

The Shock Index revisited - a fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU
- PMID: 23938104
- PMCID: PMC4057268
- DOI: 10.1186/cc12851
The Shock Index revisited - a fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU
Abstract
Introduction: Isolated vital signs (for example, heart rate or systolic blood pressure) have been shown unreliable in the assessment of hypovolemic shock. In contrast, the Shock Index (SI), defined by the ratio of heart rate to systolic blood pressure, has been advocated to better risk-stratify patients for increased transfusion requirements and early mortality. Recently, our group has developed a novel and clinical reliable classification of hypovolemic shock based upon four classes of worsening base deficit (BD). The objective of this study was to correlate this classification to corresponding strata of SI for the rapid assessment of trauma patients in the absence of laboratory parameters.
Methods: Between 2002 and 2011, data for 21,853 adult trauma patients were retrieved from the TraumaRegister DGU database and divided into four strata of worsening SI at emergency department arrival (group I, SI <0.6; group II, SI ≥0.6 to <1.0; group III, SI ≥1.0 to <1.4; and group IV, SI ≥1.4) and were assessed for demographics, injury characteristics, transfusion requirements, fluid resuscitation and outcomes. The four strata of worsening SI were compared with our recently suggested BD-based classification of hypovolemic shock.
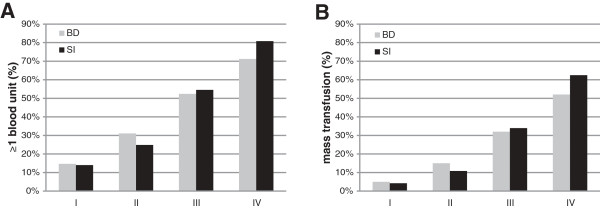
Results: Worsening of SI was associated with increasing injury severity scores from 19.3 (± 12) in group I to 37.3 (± 16.8) in group IV, while mortality increased from 10.9% to 39.8%. Increments in SI paralleled increasing fluid resuscitation, vasopressor use and decreasing hemoglobin, platelet counts and Quick's values. The number of blood units transfused increased from 1.0 (± 4.8) in group I to 21.4 (± 26.2) in group IV patients. Of patients, 31% in group III and 57% in group IV required ≥10 blood units until ICU admission. The four strata of SI discriminated transfusion requirements and massive transfusion rates equally with our recently introduced BD-based classification of hypovolemic shock.
Conclusion: SI upon emergency department arrival may be considered a clinical indicator of hypovolemic shock in respect to transfusion requirements, hemostatic resuscitation and mortality. The four SI groups have been shown to equal our recently suggested BD-based classification. In daily clinical practice, SI may be used to assess the presence of hypovolemic shock if point-of-care testing technology is not available.
Figures
Comment in
-
The Shock Index: is it ready for primetime?Crit Care. 2013 Oct 3;17(5):196. doi: 10.1186/cc13040. Crit Care. 2013. PMID: 24090407 Free PMC article.
-
Shock index: blunt clinical predictions.Crit Care. 2013 Nov 21;17(6):468. doi: 10.1186/cc13125. Crit Care. 2013. PMID: 24257460 Free PMC article. No abstract available.
-
Authors' response.Crit Care. 2013;17(6):468. Crit Care. 2013. PMID: 25320754 No abstract available.
References
-
- American College of Surgeons. Advanced Trauma Life Support for Doctors – Student Course Manual. 8. Chicago: American College of Surgeons; 2008.
-
- Mutschler M, Nienaber U, Brockamp T, Wafaisade A, Wyen H, Peiniger S, Paffrath T, Bouillon B, Maegele M. A critical reappraisal of the ATLS classification of hypovolaemic shock: does it really reflect clinical reality? Resuscitation. 2012;17:309–313. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
