

Ethnic differences in respiratory impairment
- PMID: 23939399
- PMCID: PMC3925402
- DOI: 10.1136/thoraxjnl-2013-203631
Ethnic differences in respiratory impairment
Abstract
Objective: Spirometric Z scores by lambda-mu-sigma (LMS) rigorously account for age-related changes in lung function. Recently, the Global Lung Function Initiative (GLI) expanded LMS spirometric Z scores to multiple ethnicities. Hence, in aging populations, the GLI provides an opportunity to rigorously evaluate ethnic differences in respiratory impairment, including airflow limitation and restrictive pattern.
Methods: Using data from the Third National Health and Nutrition Examination Survey, including participants aged 40-80, we evaluated ethnic differences in GLI-defined respiratory impairment, including prevalence and associations with mortality and respiratory symptoms.
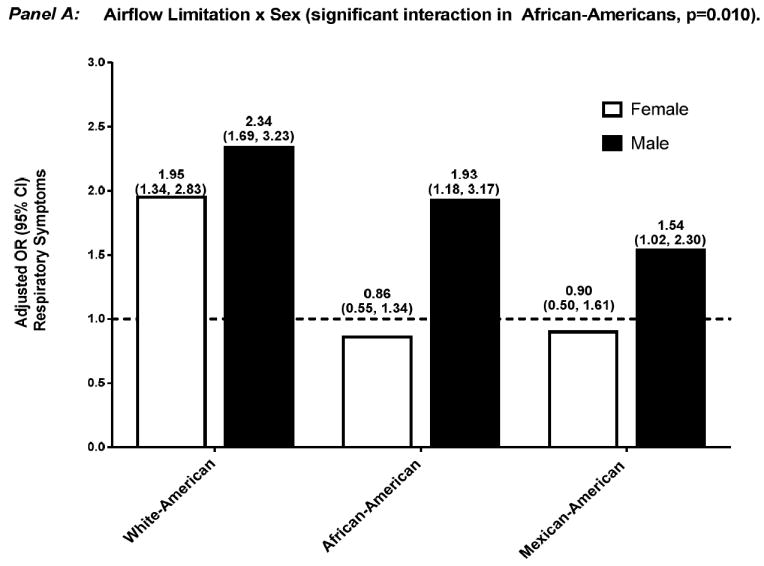
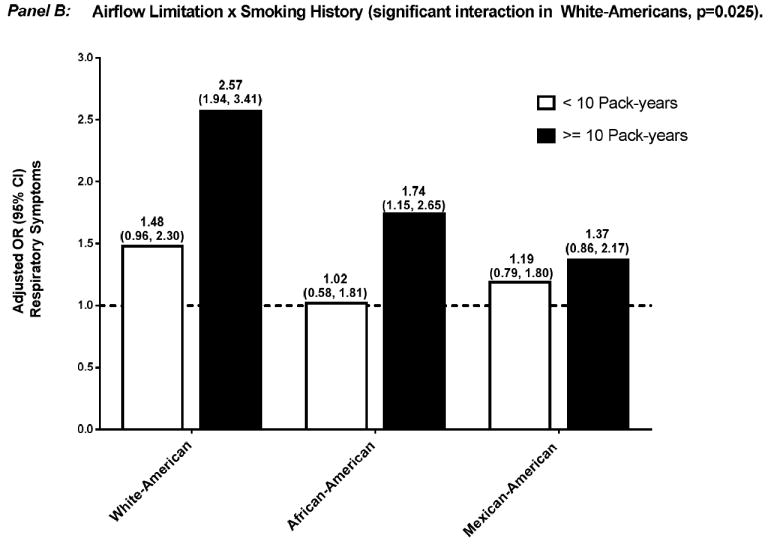
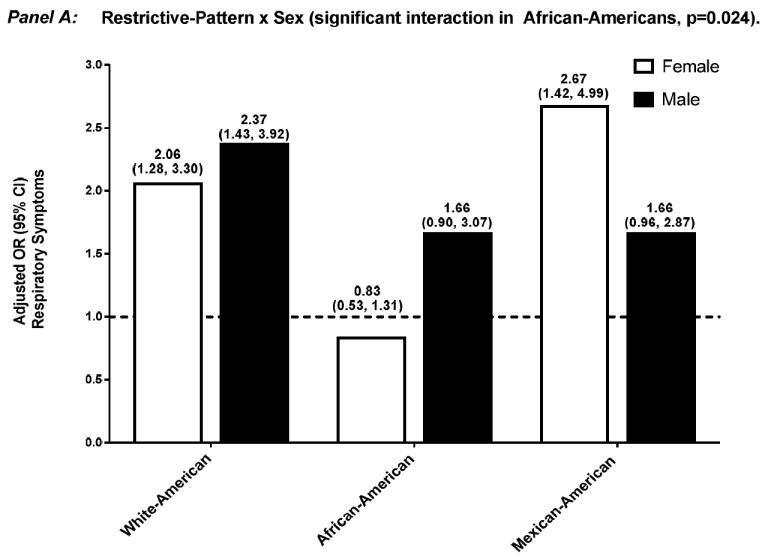
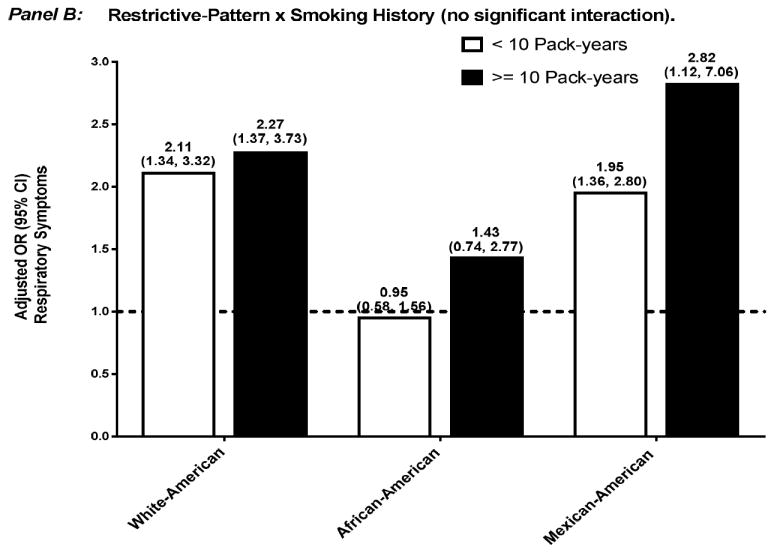
Results: Among 3506 white Americans, 1860 African Americans and 1749 Mexican Americans, the prevalence of airflow limitation was 15.1% (13.9% to 16.4%), 12.4% (10.7% to 14.0%) and 8.2% (6.7% to 9.8%), and restrictive pattern was 5.6% (4.6% to 6.5%), 8.0% (6.9% to 9.0%) and 5.7% (4.5% to 6.9%), respectively. Airflow limitation was associated with mortality in white Americans, African Americans and Mexican Americans-adjusted HR (aHR) 1.66 (1.23 to 2.25), 1.60 (1.09 to 2.36) and 1.80 (1.17 to 2.76), respectively, but associated with respiratory symptoms only in white Americans-adjusted OR (aOR) 2.15 (1.70 to 2.73). Restrictive pattern was associated with mortality but only in white Americans and African Americans-aHR 2.56 (1.84 to 3.55) and 3.23 (2.06 to 5.05), and associated with respiratory symptoms but only in white Americans and Mexican Americans-aOR 2.16 (1.51 to 3.07) and 2.12 (1.45 to 3.08), respectively.
Conclusions: In an aging population, we found ethnic differences in GLI-defined respiratory impairment. In particular, African Americans had high rates of respiratory impairment that were associated with mortality but not respiratory symptoms.
Conflict of interest statement
We report no conflicts of interest.
Figures
References
-
- Chronic Obstructive Pulmonary Disease. [03/05/2013];American Lung Association State of Lung Disease in Diverse Communities. 2010 :35–40. Available at: http://www.lung.org/assets/documents/publications/solddc-chapters/copd.pdf.
-
- Centers for Disease Control and Prevention. National Center for Health Statistics: National Health Interview Survey Raw Data, 2008. Analysis performed by American Lung Association Research and Program Services using SPSS and SUDAAN software
-
- Centers for Disease Control and Prevention. National Center for Health Statistics. 2009 CDC Wonder On-line Database, compiled from Compressed Mortality File 1999-2006 Series 20 No 2L.
-
- Miniati M, Monti S, Stolk J, et al. Value of chest radiography in phenotyping chronic obstructive pulmonary disease. Eur Respir J. 2008;31:509–14. - PubMed
-
- Peto R, Speizer FE, Cochrane AL, et al. The relevance in adults of airflow obstruction, but not of mucous hypersecretion, to mortality from chronic lung disease. Am Rev Respir Dis. 1983;128:491–500. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials