

Isolated prolactin deficiency associated with serum autoantibodies against prolactin-secreting cells
- PMID: 23940128
- PMCID: PMC3790613
- DOI: 10.1210/jc.2013-2411
Isolated prolactin deficiency associated with serum autoantibodies against prolactin-secreting cells
Erratum in
- J Clin Endocrinol Metab. 2013 Dec;98(12):4992
Abstract
Context: Isolated prolactin (PRL) deficiency is a rare entity of unknown etiology manifesting as failure of puerperal lactogenesis.
Objective: The aim of the study was to determine the cause of isolated PRL deficiency in an affected woman.
Design and setting: We examined genetic and autoimmune causes of isolated PRL deficiency at academic medical centers.
Patient: The patient was a 39-year-old woman with puerperal alactogenesis after two deliveries and undetectable PRL. The other pituitary axes, serum calcium levels, and cranial magnetic resonance imaging were normal.
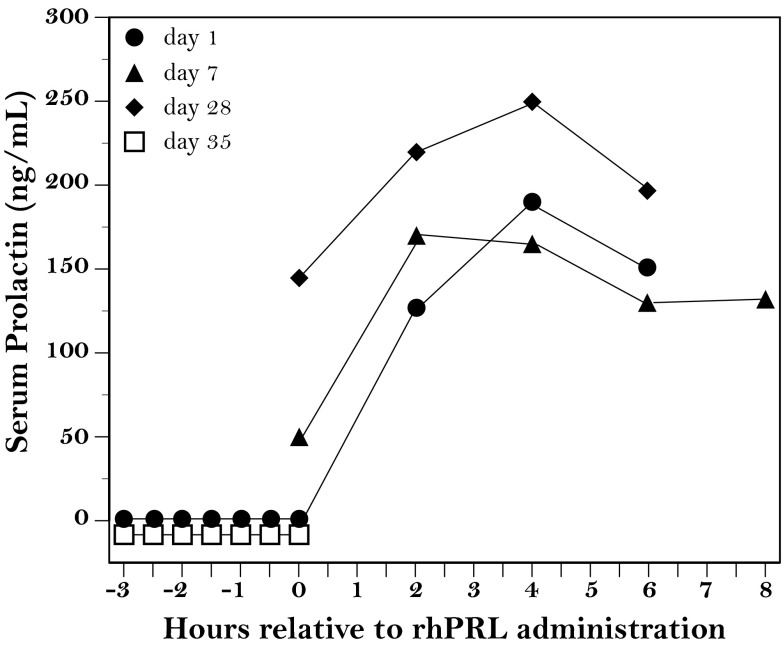
Intervention: Recombinant human PRL (r-hPRL) was administered to the patient.
Main outcome measures: We measured the sequencing of candidate genes and immunofluorescence analysis of autoantibodies directed against pituitary endocrine cells.
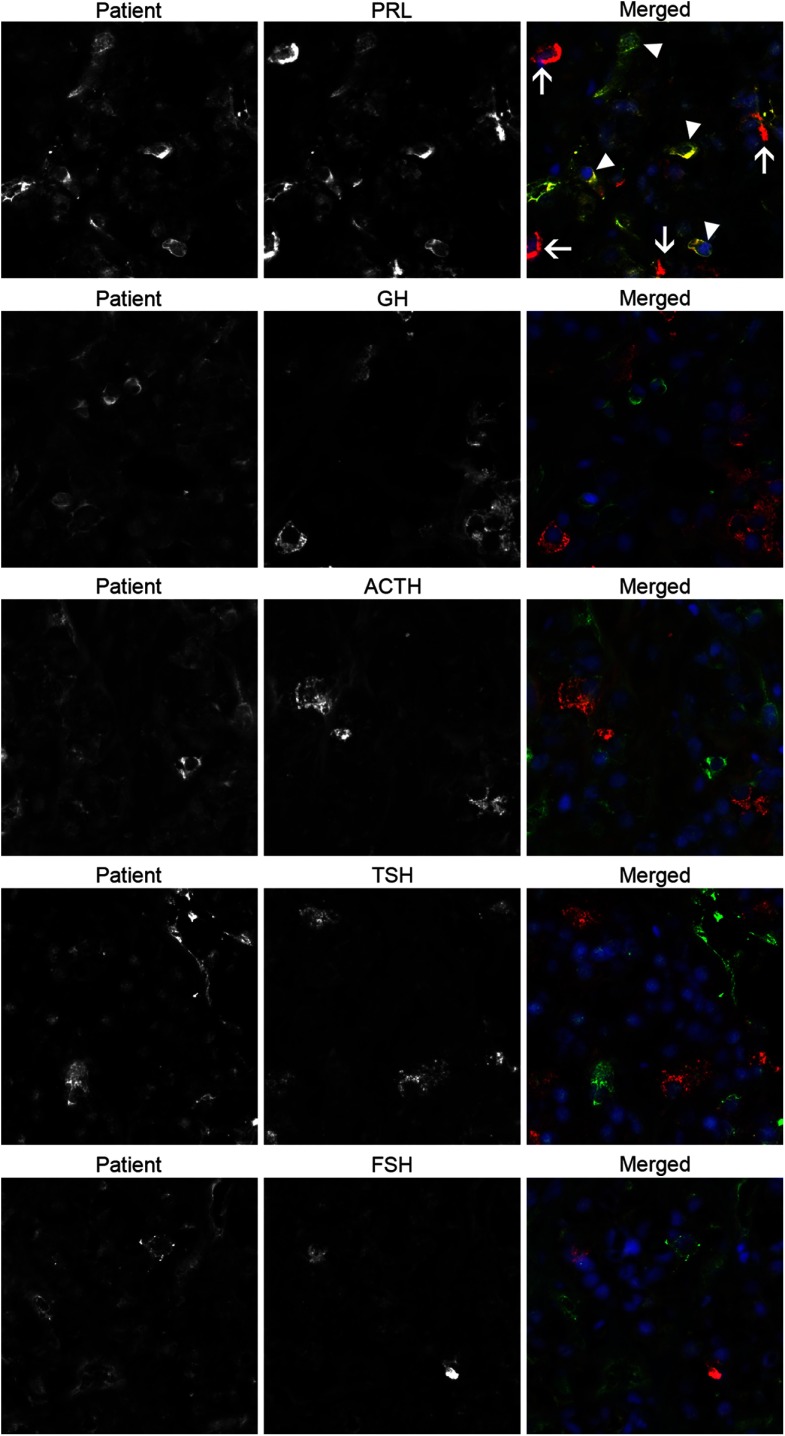
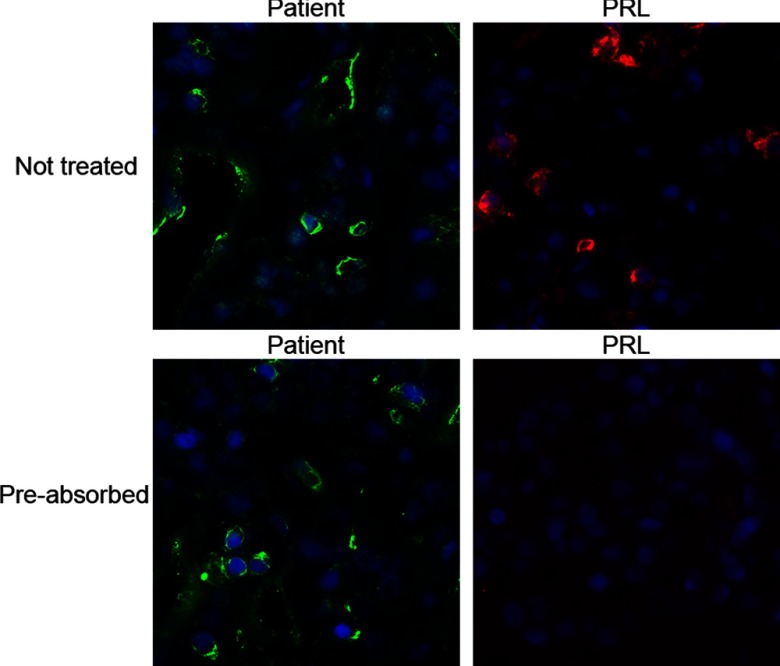
Results: There were no rare sequence variants in the genes encoding for PRL, putative PRL-releasing peptide, putative PRL-releasing peptide receptor, or in other genes important for lactotroph lineage development (POU1F1, PROP1, LHX3, LHX4, HESX1, OTX2, and LSD1). The patient serum, on the contrary, contained autoantibodies that specifically recognized a subset of PRL-secreting cells but not PRL itself or any other pituitary cells or hormones. The mother was able to lactate fully after 17 days of treatment with r-hPRL 60 μg/kg every 12 hours, but alactogenesis resumed after treatment was completed.
Conclusions: These studies report a new autoimmune etiology for women with isolated PRL deficiency and puerperal alactogenesis.
Trial registration: ClinicalTrials.gov NCT00181623.
Figures
References
-
- Toledano Y, Lubetsky A, Shimon I. Acquired prolactin deficiency in patients with disorders of the hypothalamic-pituitary axis. J Endocrinol Invest. 2007;30:268–273 - PubMed
-
- Carlson HE, Brickman AS, Bottazzo GF. Prolactin deficiency in pseudohypoparathyroidism. N Engl J Med. 1977;296:140–144 - PubMed
-
- Prince KL, Walvoord EC, Rhodes SJ. The role of homeodomain transcription factors in heritable pituitary disease. Nat Rev Endocrinol. 2011;7:727–737 - PubMed
-
- Romero CJ, Pine-Twaddell E, Radovick S. Novel mutations associated with combined pituitary hormone deficiency. J Mol Endocrinol. 2011;46:R93–R102 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
