

Definitive results of a phase III adjuvant trial comparing three chemotherapy regimens in women with operable, node-positive breast cancer: the NSABP B-38 trial
- PMID: 23940225
- PMCID: PMC3757290
- DOI: 10.1200/JCO.2012.48.1275
Definitive results of a phase III adjuvant trial comparing three chemotherapy regimens in women with operable, node-positive breast cancer: the NSABP B-38 trial
Abstract
Purpose: Anthracycline- and taxane-based three-drug chemotherapy regimens have proven benefit as adjuvant therapy for early-stage breast cancer. This trial (NSABP B-38; Combination Chemotherapy in Treating Women Who Have Undergone Surgery for Node-Positive Breast Cancer) asked whether the incorporation of a fourth drug could improve outcomes relative to two standard regimens and provided a direct comparison of those two regimens.
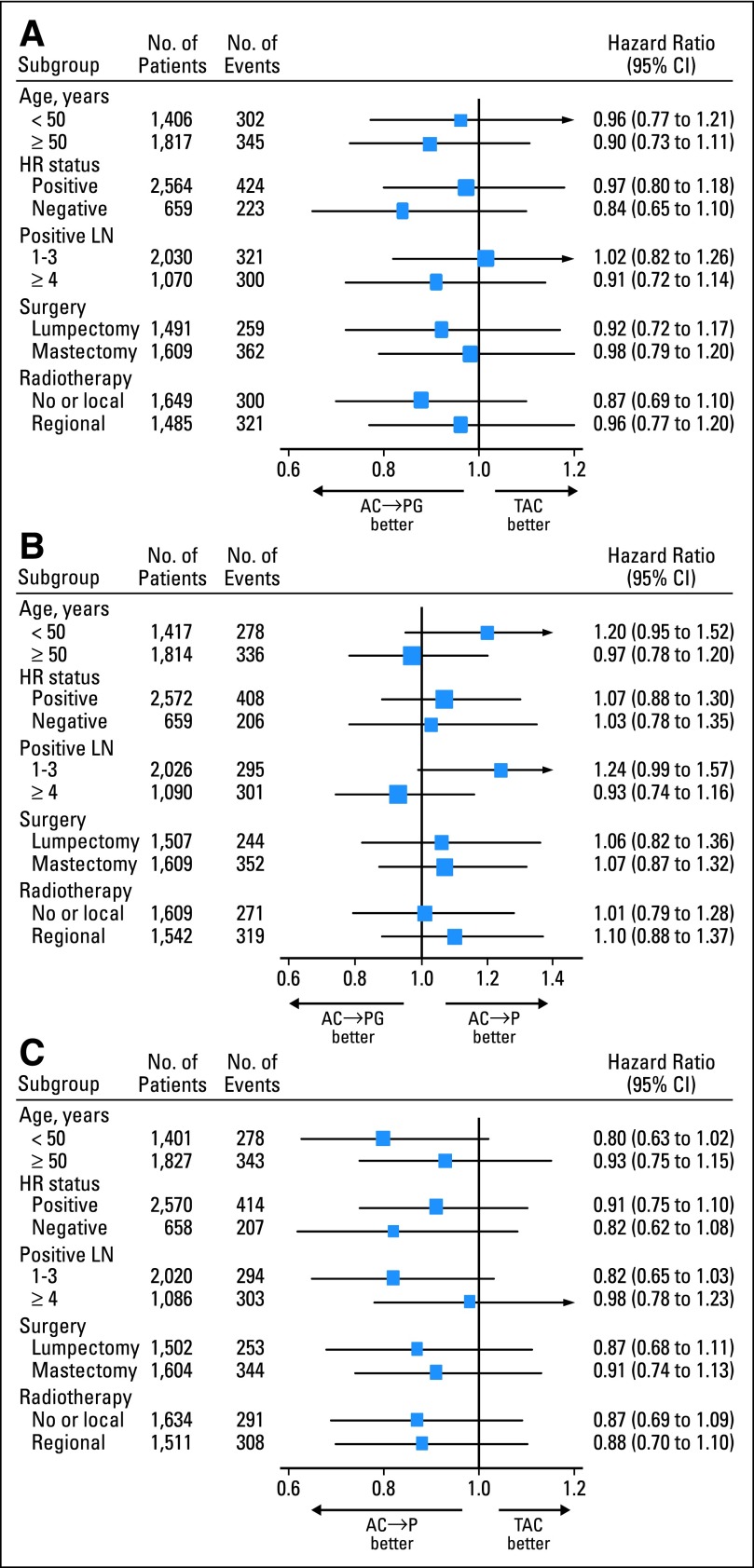
Patients and methods: We randomly assigned 4,894 women with node-positive early-stage breast cancer to six cycles of docetaxel, doxorubicin, and cyclophosphamide (TAC), four cycles of dose-dense (DD) doxorubicin and cyclophosphamide followed by four cycles of DD paclitaxel (P; DD AC→P), or DD AC→P with four cycles of gemcitabine (G) added to the DD paclitaxel (DD AC→PG). Primary granulocyte colony-stimulating factor support was required; erythropoiesis-stimulating agents (ESAs) were used at the investigator's discretion.
Results: There were no significant differences in 5-year disease-free survival (DFS) between DD AC→PG and DD AC→P (80.6% v 82.2%; HR, 1.07; P = .41), between DD AC→PG and TAC (80.6% v 80.1%; HR, 0.93; P = .39), in 5-year overall survival (OS) between DD AC→PG and DD AC→P (90.8% v 89.1%; HR, 0.85; P = .13), between DD AC→PG and TAC (90.8% v 89.6%; HR, 0.86; P = .17), or between DD AC→P versus TAC for DFS (HR, 0.87; P = .07) and OS (HR, 1.01; P = .96). Grade 3 to 4 toxicities for TAC, DD AC→P, and DD AC→PG, respectively, were febrile neutropenia (9%, 3%, 3%; P < .001), sensory neuropathy (< 1%, 7%, 6%; P < .001), and diarrhea (7%, 2%, 2%; P < .001). Exploratory analyses for ESAs showed no association with DFS events (HR, 1.02; P = .95).
Conclusion: Adding G to DD AC→P did not improve outcomes. No significant differences in efficacy were identified between DD AC→P and TAC, although toxicity profiles differed.
Trial registration: ClinicalTrials.gov NCT00093795.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures








Comment in
-
Are dose-dense and triplet chemotherapy regimens optimal adjuvant therapy in the majority of women with node-positive early breast cancer?J Clin Oncol. 2014 Feb 20;32(6):605-6. doi: 10.1200/JCO.2013.53.6771. Epub 2014 Jan 13. J Clin Oncol. 2014. PMID: 24419118 No abstract available.
-
Reply to E.J. Moylan et al.J Clin Oncol. 2014 Feb 20;32(6):606-7. doi: 10.1200/JCO.2013.53.8744. Epub 2014 Jan 13. J Clin Oncol. 2014. PMID: 24419136 Free PMC article. No abstract available.
References
-
- Henderson IC, Berry DA, Demetri GD, et al. Improved outcomes from adding sequential paclitaxel but not from escalating doxorubicin dose in an adjuvant chemotherapy regimen for patients with node-positive primary breast cancer. J Clin Oncol. 2003;21:976–983. - PubMed
-
- Citron ML, Berry DA, Cirrincione C, et al. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: First report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J Clin Oncol. 2003;21:1431–1439. - PubMed
-
- Martin M, Pienkowski T, Mackey J, et al. Adjuvant docetaxel for node-positive breast cancer. N Engl J Med. 2005;352:2302–2313. - PubMed
-
- Mamounas EP, Bryant J, Lembersky B, et al. Paclitaxel after doxorubicin plus cyclophosphamide as adjuvant chemotherapy for node-positive breast cancer: Results from NSABP B-28. J Clin Oncol. 2005;23:3686–3696. - PubMed
-
- Roché H, Fumoleau P, Spielmann M, et al. Sequential adjuvant epirubicin-based and docetaxel chemotherapy for node-positive breast cancer patients: The FNCLCC PACS 01 Trial. J Clin Oncol. 2006;24:5664–5671. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10-CA-69651/CA/NCI NIH HHS/United States
- U10-CA-25224/CA/NCI NIH HHS/United States
- U10-CA-37377/CA/NCI NIH HHS/United States
- U10 CA012027/CA/NCI NIH HHS/United States
- P30 CA051008/CA/NCI NIH HHS/United States
- U10 CA069651/CA/NCI NIH HHS/United States
- U10 CA069974/CA/NCI NIH HHS/United States
- U10 CA044066/CA/NCI NIH HHS/United States
- U10 CA025224/CA/NCI NIH HHS/United States
- CA44066-25/CA/NCI NIH HHS/United States
- U10 CA037377/CA/NCI NIH HHS/United States
- U10-CA-69974/CA/NCI NIH HHS/United States
- U10-CA-12027/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
