

Detection of obstructive coronary artery disease using regadenoson stress and 82Rb PET/CT myocardial perfusion imaging
- PMID: 23940305
- PMCID: PMC4382359
- DOI: 10.2967/jnumed.113.120063
Detection of obstructive coronary artery disease using regadenoson stress and 82Rb PET/CT myocardial perfusion imaging
Abstract
Our objective was to study the diagnostic performance of regadenoson (82)Rb myocardial perfusion PET imaging to detect obstructive coronary artery disease (CAD).
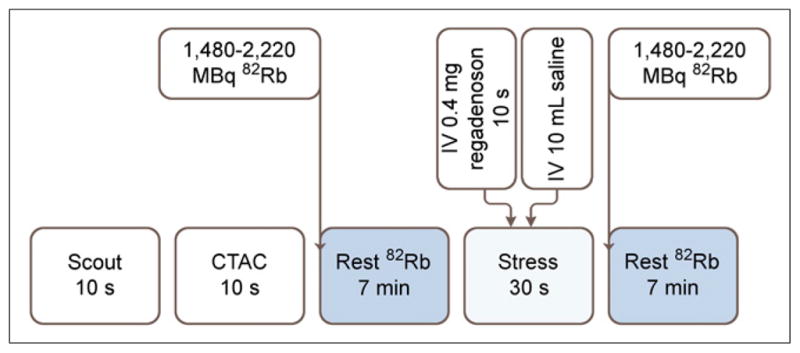
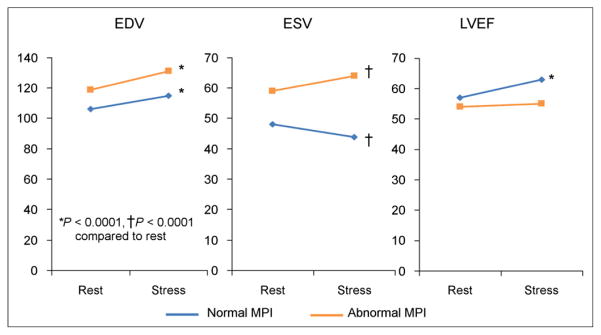
Methods: We studied 134 patients (mean age, 63 ± 12 y; mean body mass index, 31 ± 9 kg/m(2)) without known CAD (96 with coronary angiography and 38 with low pretest likelihood of CAD). Stress left ventricular ejection fraction (LVEF) minus rest LVEF defined LVEF reserve. The Duke score was used to estimate the anatomic extent of jeopardized myocardium.
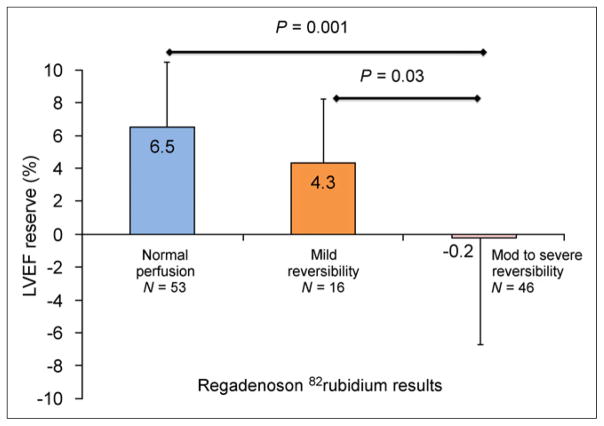
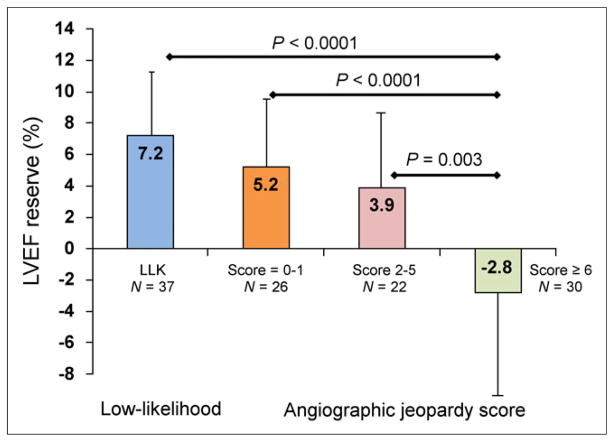
Results: Regadenoson PET had a high sensitivity, 92% (95% confidence interval [CI], 83%-97%), in detecting obstructive CAD, with a normalcy rate of 97% (95% CI, 86%-99%), specificity of 77% (54/70 patients; 95% CI, 66%-86%), and area under the receiver-operator-characteristic curve of 0.847 (95% CI, 0.774-0.903; P < 0.001). Regadenoson PET demonstrated high sensitivity to detect CAD in patients with single-vessel CAD (89%; 95% CI, 70%-98%). The mean LVEF reserve was significantly higher in patients with normal myocardial perfusion imaging results (6.5% ± 5.4%) than in those with mild (4.3 ± 5.1, P = 0.03) and moderate to severe reversible defects (-0.2% ± 8.4%, P = 0.001). Also, mean LVEF reserve was significantly higher in patients with a low likelihood of CAD (7.2% ± 4.5%, P < 0.0001) and mild or moderate jeopardized myocardium than in those with significant jeopardized myocardium (score ≥ 6), -2.8% ± 8.3%.
Conclusion: Regadenoson (82)Rb myocardial perfusion imaging is accurate for the detection of obstructive CAD. LVEF reserve is high in patients without significant ischemia or significant angiographic jeopardized myocardium.
Keywords: 82Rb; coronary angiography; diagnostic accuracy; ejection fraction; regadenoson.
Figures

References
-
- Cerqueira MD, Nguyen P, Staehr P, Underwood SR, Iskandrian AE. Effects of age, gender, obesity, and diabetes on the efficacy and safety of the selective A2A agonist regadenoson versus adenosine in myocardial perfusion imaging integrated ADVANCE-MPI trial results. JACC Cardiovasc Imaging. 2008;1:307–316. - PubMed
-
- Iskandrian AE, Bateman TM, Belardinelli L, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol. 2007;14:645–658. - PubMed
-
- Mahmarian JJ, Cerqueira MD, Iskandrian AE, et al. Regadenoson induces comparable left ventricular perfusion defects as adenosine: a quantitative analysis from the ADVANCE MPI 2 trial. JACC Cardiovasc Imaging. 2009;2:959–968. - PubMed
-
- Lieu HD, Shryock JC, von Mering GO, et al. Regadenoson, a selective A2A adenosine receptor agonist, causes dose-dependent increases in coronary blood flow velocity in humans. J Nucl Cardiol. 2007;14:514–520. - PubMed
-
- Di Carli MF, Hachamovitch R. New technology for noninvasive evaluation of coronary artery disease. Circulation. 2007;115:1464–1480. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous