

Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism
- PMID: 23940438
- PMCID: PMC3718593
Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism
Abstract
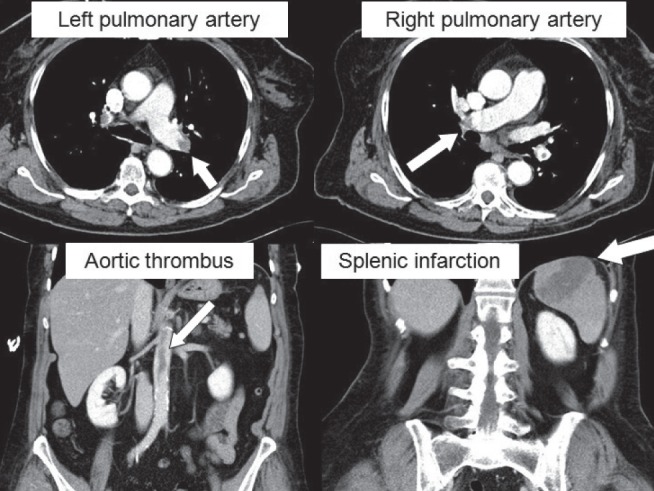
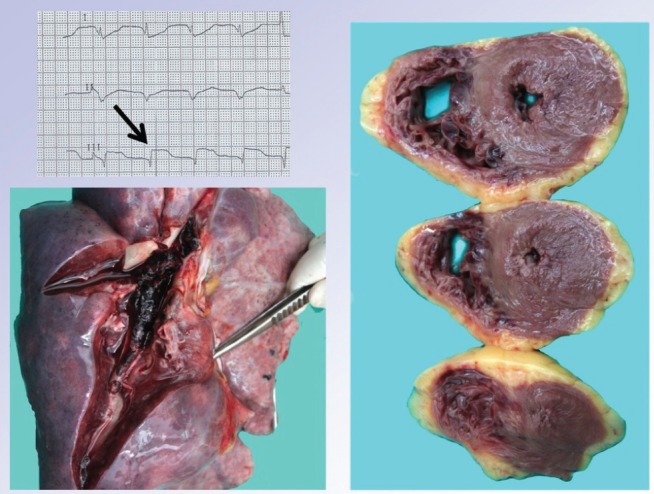
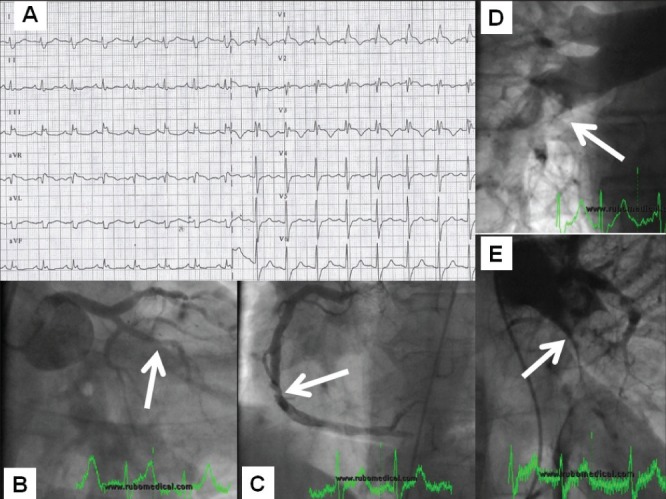
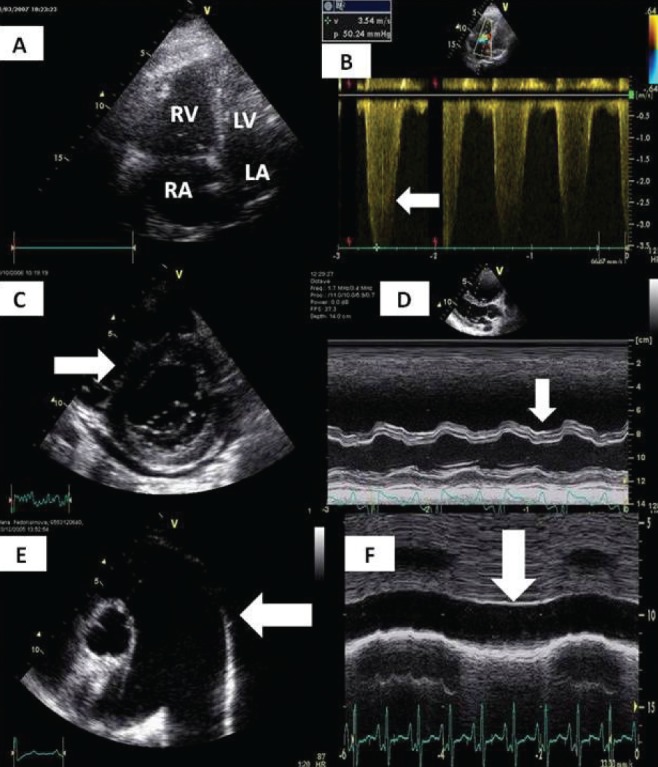
Pulmonary embolism is an important clinical entity with considerable mortality despite advances in diagnosis and treatment. In the present article, the authors offer a comprehensive review focused mainly on epidemiology, risk factors, risk stratification, pathophysiological considerations and clinical presentation. Diagnosis based on assessment of clinical likelihood, electrocardiography, chest x-ray, D-dimer levels, markers of myocardial injury and overload, and blood gases is discussed in detail. Special attention is devoted to the clinical use of computed tomography, pulmonary angiography and echocardiography in the setting of pulmonary embolism.
Keywords: Diagnosis; Epidemiology; Pulmonary embolism; Risk stratification.
Figures

References
-
- Oger E. Incidence of venous thromboembolism in a community-based study in western France. Thromb Haemost. 2000;83:657–60. - PubMed
-
- Widimský J, Malý J, Eliáš P, et al. Doporučení pro diagnostiku a léčbu akutní plicní embolie. Vnitř. Lék. 2008;54:1S25–1S72.
-
- Torbicki A, Perrier A, Konstantidines S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2008;29:2276–315. - PubMed
-
- Meignan M, Rosso J, Gauthier H, et al. Systematic lung scans reveal a high frequency of silent pulmonary embolism in patients with proximal deep venous thrombosis. Arch Intern Med. 2000;160:159–64. - PubMed
-
- Pineda LA, Hathwar VS, Grant BJ. Clinical suspicion of fatal pulmonary embolism. Chest. 2001;120:791–5. - PubMed
LinkOut - more resources
Full Text Sources
Medical