

Switching HIV treatment in adults based on CD4 count versus viral load monitoring: a randomized, non-inferiority trial in Thailand
- PMID: 23940461
- PMCID: PMC3735458
- DOI: 10.1371/journal.pmed.1001494
Switching HIV treatment in adults based on CD4 count versus viral load monitoring: a randomized, non-inferiority trial in Thailand
Abstract
Background: Viral load (VL) is recommended for monitoring the response to highly active antiretroviral therapy (HAART) but is not routinely available in most low- and middle-income countries. The purpose of the study was to determine whether a CD4-based monitoring and switching strategy would provide a similar clinical outcome compared to the standard VL-based strategy in Thailand.
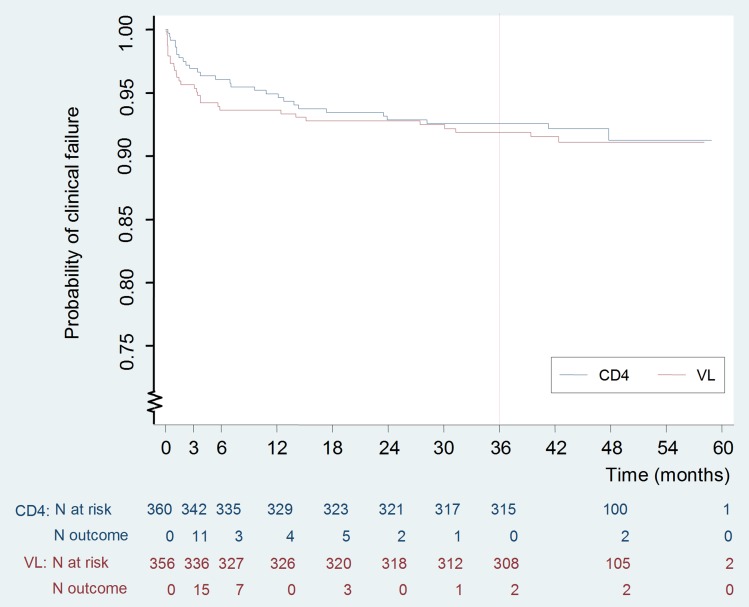
Methods and findings: The Programs for HIV Prevention and Treatment (PHPT-3) non-inferiority randomized clinical trial compared a treatment switching strategy based on CD4-only (CD4) monitoring versus viral-load (VL). Consenting participants were antiretroviral-naïve HIV-infected adults (CD4 count 50-250/mm(3)) initiating non-nucleotide reverse transcriptase inhibitor (NNRTI)-based therapy. Randomization, stratified by site (21 public hospitals), was performed centrally after enrollment. Clinicians were unaware of the VL values of patients randomized to the CD4 arm. Participants switched to second-line combination with confirmed CD4 decline >30% from peak (within 200 cells from baseline) in the CD4 arm, or confirmed VL >400 copies/ml in the VL arm. Primary endpoint was clinical failure at 3 years, defined as death, new AIDS-defining event, or CD4 <50 cells/mm(3). The 3-year Kaplan-Meier cumulative risks of clinical failure were compared for non-inferiority with a margin of 7.4%. In the intent to treat analysis, data were censored at the date of death or at last visit. The secondary endpoints were difference in future-drug-option (FDO) score, a measure of resistance profiles, virologic and immunologic responses, and the safety and tolerance of HAART. 716 participants were randomized, 356 to VL monitoring and 360 to CD4 monitoring. At 3 years, 319 participants (90%) in VL and 326 (91%) in CD4 were alive and on follow-up. The cumulative risk of clinical failure was 8.0% (95% CI 5.6-11.4) in VL versus 7.4% (5.1-10.7) in CD4, and the upper-limit of the one-sided 95% CI of the difference was 3.4%, meeting the pre-determined non-inferiority criterion. Probability of switch for study criteria was 5.2% (3.2-8.4) in VL versus 7.5% (5.0-11.1) in CD4 (p=0.097). Median time from treatment initiation to switch was 11.7 months (7.7-19.4) in VL and 24.7 months (15.9-35.0) in CD4 (p=0.001). The median duration of viremia >400 copies/ml at switch was 7.2 months (5.8-8.0) in VL versus 15.8 months (8.5-20.4) in CD4 (p=0.002). FDO scores were not significantly different at time of switch. No adverse events related to the monitoring strategy were reported.
Conclusions: The 3-year rates of clinical failure and loss of treatment options did not differ between strategies although the longer-term consequences of CD4 monitoring would need to be investigated. These results provide reassurance to treatment programs currently based on CD4 monitoring as VL measurement becomes more affordable and feasible in resource-limited settings.
Trial registration: ClinicalTrials.govNCT00162682 Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Egger M, May M, Chene G, Phillips AN, Ledergerber B, et al. (2002) Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet 360: 119–129. - PubMed
-
- Thompson MA, Aberg JA, Cahn P, Montaner JS, Rizzardini G, et al. (2010) Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA 304: 321–333. - PubMed
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents (2011). Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Washington (D.C.): Department of Health and Human Services. October 14, 2011. pp. 1–167.
-
- World Health Organization (2013). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Recommendations for a public health approach. June 2013. Geneva: WHO. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
