

The relationship between baseline nutritional status with subsequent parenteral nutrition and clinical outcomes in cancer patients undergoing hyperthermic intraperitoneal chemotherapy
- PMID: 23941331
- PMCID: PMC3751179
- DOI: 10.1186/1475-2891-12-118
The relationship between baseline nutritional status with subsequent parenteral nutrition and clinical outcomes in cancer patients undergoing hyperthermic intraperitoneal chemotherapy
Abstract
Background: The combination of cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) is a promising treatment option for selected patients with peritoneal carcinomatosis. This retrospective study investigated the relationship between baseline nutritional assessment with subsequent parenteral nutritional (PN) and clinical outcomes in cancer patients undergoing CRS and HIPEC.
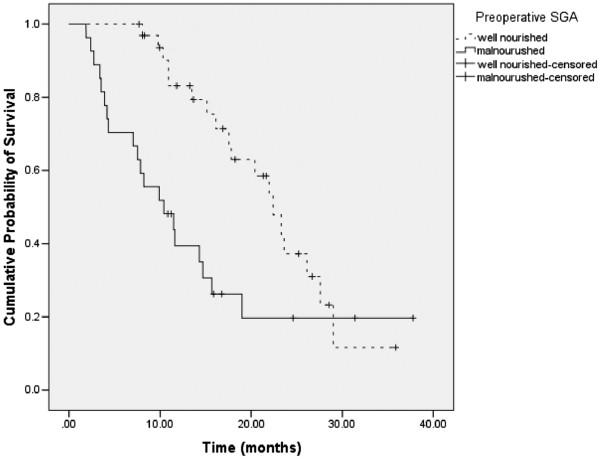
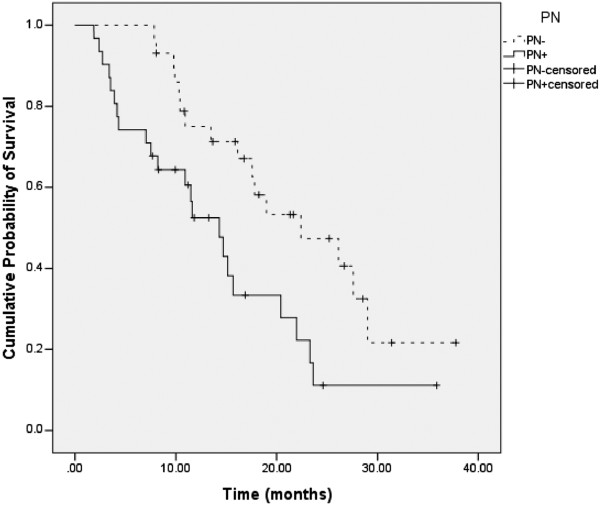
Methods: A consecutive series of 60 patients undergoing CRS and HIPEC at our institution between January 2009 and May 2011. Subjective Global Assessment (SGA) was used to assess nutritional status. Patients were classified preoperatively as: well nourished (SGA-A), mildly-moderately malnourished (SGA-B), and severely malnourished (SGA-C). For PN, patients were divided into 2 groups: those who received PN (PN+) and those who did not receive PN (PN-). The primary outcomes of interest were length of stay (LOS), postoperative complications, ECOG performance status (PS) and survival. LOS was calculated as the number of days in the hospital post surgery. Performance status was measured on a scale of 0-4. Survival was calculated from the date of first visit to the date of death/last contact.
Results: Of 60 patients, 19 were males and 41 females. The mean age at presentation was 50.3 years. The most common cancer types were colorectal (n = 24) and gynecologic (n = 19) with the majority of patients (n = 47) treated previously before coming to our institution. 33 patients were SGA-A, 22 SGA-B and 5 SGA-C prior to surgery. Of a total of 60 patients, 31 received PN. Mean LOS for the entire cohort was 16.2 days (SD = 9.8). Mean LOS for preoperative SGA-A, SGA-B and SGA-C were 15.0, 15.2 and 27.8 days respectively (ANOVA p = 0.02). Overall incidence of complications was 26.7% (16/60). Complications were recorded in 9 of 33 (27.3%) preoperative SGA-A patients and 7 of 27 (25.9%) SGA-B + C patients (p = 0.91). The median overall survival was 17.5 months (95% CI = 13.0 to 22.1 months). Median survival for preoperative SGA-A and SGA-B + C cohorts was 22.4 and 10.4 months respectively (p = 0.006).
Conclusions: The preoperative SGA predicts LOS and survival in cancer patients undergoing HIPEC. Future randomized clinical trials in this patient population should investigate the systematic provision of PN to all malnourished patients in the preoperative period for a minimum of 7-10 days with the continuation of PN in the postoperative period.
Figures
Similar articles
-
Preoperative Nutrition Status and Postoperative Outcomes in Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy.Ann Surg Oncol. 2019 Aug;26(8):2622-2630. doi: 10.1245/s10434-019-07415-7. Epub 2019 May 23. Ann Surg Oncol. 2019. PMID: 31123932
-
Parenteral nutrition after cytoreductive surgery for peritoneal malignancy: Should it be administered routinely?Clin Nutr ESPEN. 2023 Oct;57:487-493. doi: 10.1016/j.clnesp.2023.06.016. Epub 2023 Jul 26. Clin Nutr ESPEN. 2023. PMID: 37739696
-
Perioperative nutritional assessment and interventions in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC): A systematic review.Eur J Surg Oncol. 2023 May;49(5):902-917. doi: 10.1016/j.ejso.2023.02.015. Epub 2023 Feb 27. Eur J Surg Oncol. 2023. PMID: 36872111
-
[Efficacy of 1 384 cases of peritoneal carcinomatosis underwent cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Mar 25;24(3):230-239. doi: 10.3760/cma.j.cn.441530-20201110-00603. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 34645167 Chinese.
-
The Role of Preoperative Parenteral Nutrition.Nutrients. 2020 May 6;12(5):1320. doi: 10.3390/nu12051320. Nutrients. 2020. PMID: 32384662 Free PMC article.
Cited by
-
The relationship between baseline nutritional status with subsequent parenteral nutrition and clinical outcomes in cancer patients undergoing cytoreductive surgery: a retrospective study.Front Nutr. 2024 May 3;11:1364959. doi: 10.3389/fnut.2024.1364959. eCollection 2024. Front Nutr. 2024. PMID: 38765813 Free PMC article.
-
The Clinical Importance of Preoperative Rectal Swabs in Patients after Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy.Visc Med. 2022 Dec;38(6):376-383. doi: 10.1159/000526001. Epub 2022 Aug 18. Visc Med. 2022. PMID: 36589250 Free PMC article.
-
Systematic review and meta-analysis of the evidence for oral nutritional intervention on nutritional and clinical outcomes during chemo(radio)therapy: current evidence and guidance for design of future trials.Ann Oncol. 2018 May 1;29(5):1141-1153. doi: 10.1093/annonc/mdy114. Ann Oncol. 2018. PMID: 29788170 Free PMC article.
-
The influence of preoperative nutritional status on the outcomes of an enhanced recovery after surgery (ERAS) programme for colorectal cancer surgery.Tech Coloproctol. 2014 Nov;18(11):1075-80. doi: 10.1007/s10151-014-1210-4. Epub 2014 Sep 13. Tech Coloproctol. 2014. PMID: 25216721
-
Prognostication of Survival in Patients With Advanced Cancer: Predicting the Unpredictable?Cancer Control. 2015 Oct;22(4):489-97. doi: 10.1177/107327481502200415. Cancer Control. 2015. PMID: 26678976 Free PMC article. Review.
References
-
- Deraco M, Baratti D, Laterza B, Balestra MR, Mingrone E, Macri A. et al.Advanced cytoreduction as surgical standard of care and hyperthermic intraperitoneal chemotherapy as promising treatment in epithelial ovarian cancer. Eur J Surg Oncol. 2011;37:4–9. doi: 10.1016/j.ejso.2010.11.004. - DOI - PubMed
-
- Glehen O, Gilly FN, Arvieux C, Cotte E, Boutitie F, Mansvelt B. et al.Peritoneal carcinomatosis from gastric cancer: a multi-institutional study of 159 patients treated by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Ann Surg Oncol. 2010;17:2370–2377. doi: 10.1245/s10434-010-1039-7. - DOI - PubMed
-
- Hagendoorn J, van Lammeren G, Boerma D, van der BE, Wiezer MJ, van Ramshorst B. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis from colorectal and gastrointestinal origin shows acceptable morbidity and high survival. Eur J Surg Oncol. 2009;35:833–837. doi: 10.1016/j.ejso.2008.10.006. - DOI - PubMed
-
- Pavlov MJ, Kovacevic PA, Ceranic MS, Stamenkovic AB, Ivanovic AM, Kecmanovic DM. Cytoreductive surgery and modified heated intraoperative intraperitoneal chemotherapy (HIPEC) for advanced and recurrent ovarian cancer – 12-year single center experience. Eur J Surg Oncol. 2009;35:1186–1191. doi: 10.1016/j.ejso.2009.03.004. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
