

Balancing the rates of new bone formation and polymer degradation enhances healing of weight-bearing allograft/polyurethane composites in rabbit femoral defects
- PMID: 23941405
- PMCID: PMC3875200
- DOI: 10.1089/ten.TEA.2012.0762
Balancing the rates of new bone formation and polymer degradation enhances healing of weight-bearing allograft/polyurethane composites in rabbit femoral defects
Abstract
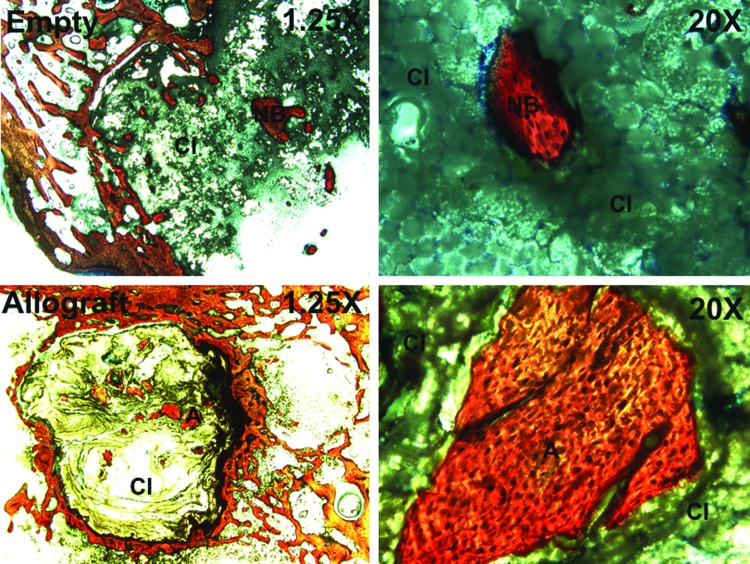
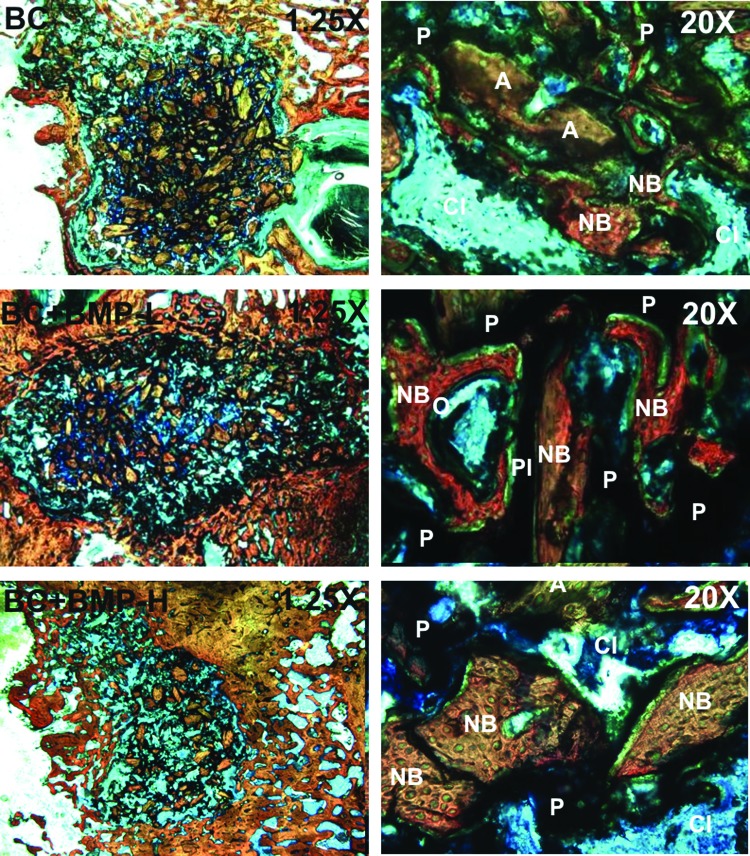
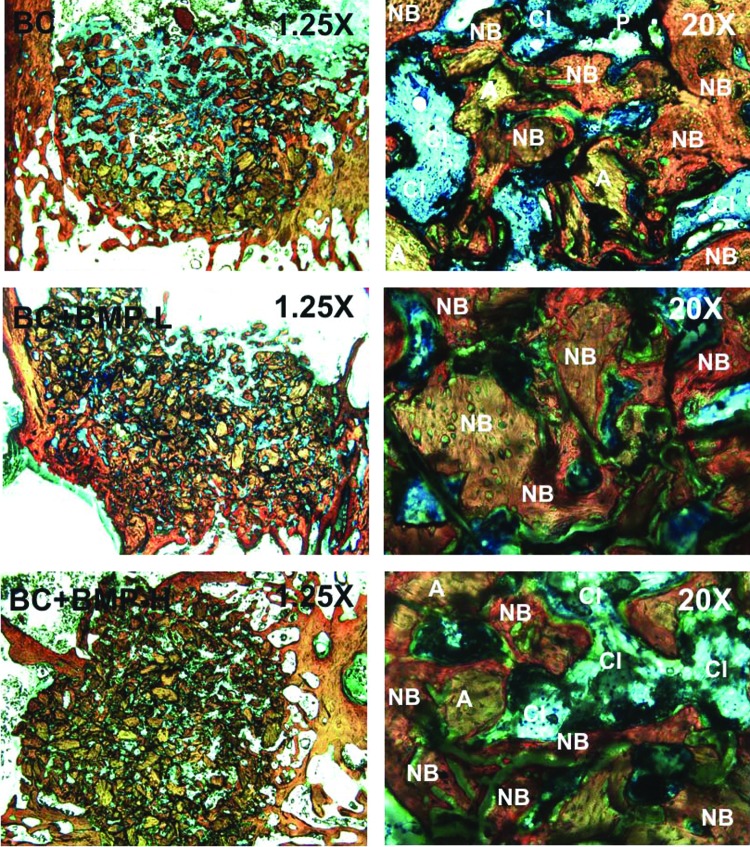
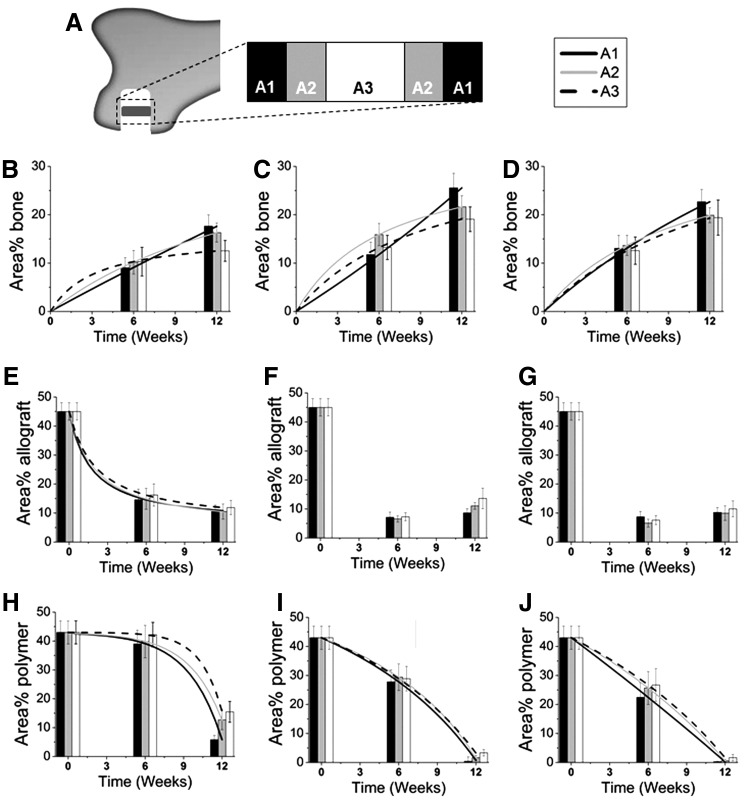
There is a compelling clinical need for bone grafts with initial bone-like mechanical properties that actively remodel for repair of weight-bearing bone defects, such as fractures of the tibial plateau and vertebrae. However, there is a paucity of studies investigating remodeling of weight-bearing bone grafts in preclinical models, and consequently there is limited understanding of the mechanisms by which these grafts remodel in vivo. In this study, we investigated the effects of the rates of new bone formation, matrix resorption, and polymer degradation on healing of settable weight-bearing polyurethane/allograft composites in a rabbit femoral condyle defect model. The grafts induced progressive healing in vivo, as evidenced by an increase in new bone formation, as well as a decrease in residual allograft and polymer from 6 to 12 weeks. However, the mismatch between the rates of autocatalytic polymer degradation and zero-order (independent of time) new bone formation resulted in incomplete healing in the interior of the composite. Augmentation of the grafts with recombinant human bone morphogenetic protein-2 not only increased the rate of new bone formation, but also altered the degradation mechanism of the polymer to approximate a zero-order process. The consequent matching of the rates of new bone formation and polymer degradation resulted in more extensive healing at later time points in all regions of the graft. These observations underscore the importance of balancing the rates of new bone formation and degradation to promote healing of settable weight-bearing bone grafts that maintain bone-like strength, while actively remodeling.
Figures
References
-
- Russell T.A., and Leighton R.K.Comparison of autogenous bone graft and endothermic calcium phosphate cement for defect augmentation in tibial plateau fractures. A multicenter, prospective, randomized study. J Bone Joint Surg Am 90, 2057, 2008. Epub 2008/10/03. - PubMed
-
- Simpson D., and Keating J.F.Outcome of tibial plateau fractures managed with calcium phosphate cement. Injury 35, 913, 2004. Epub 2004/08/11. - PubMed
-
- Hall J.A., Beuerlein M.J., and McKee M.D.Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am 91 Suppl 2 (Pt 1), 74, 2009. Epub 2009/03/11. - PubMed
-
- Schwartz Z., Goldstein M., Raviv E., Hirsch A., Ranly D.M., and Boyan B.D.Clinical evaluation of demineralized bone allograft in a hyaluronic acid carrier for sinus lift augmentation in humans: a computed tomography and histomorphometric study. Clin Oral Implants Res 18, 204, 2007. Epub 2007/03/14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
