

Exosomes carrying mycobacterial antigens can protect mice against Mycobacterium tuberculosis infection
- PMID: 23943377
- PMCID: PMC4076847
- DOI: 10.1002/eji.201343727
Exosomes carrying mycobacterial antigens can protect mice against Mycobacterium tuberculosis infection
Abstract
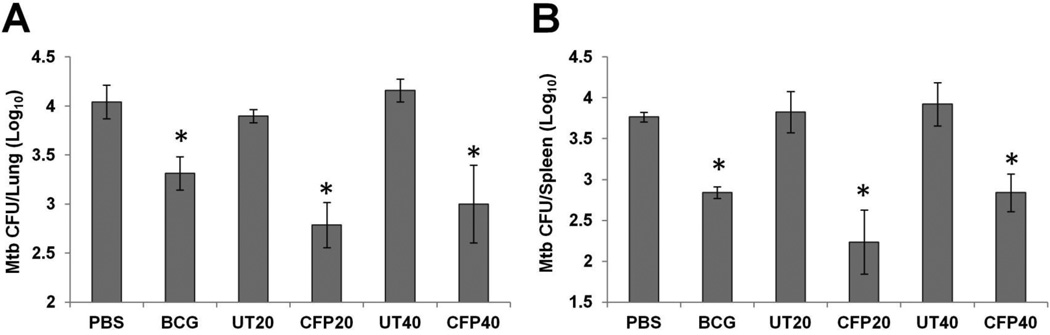
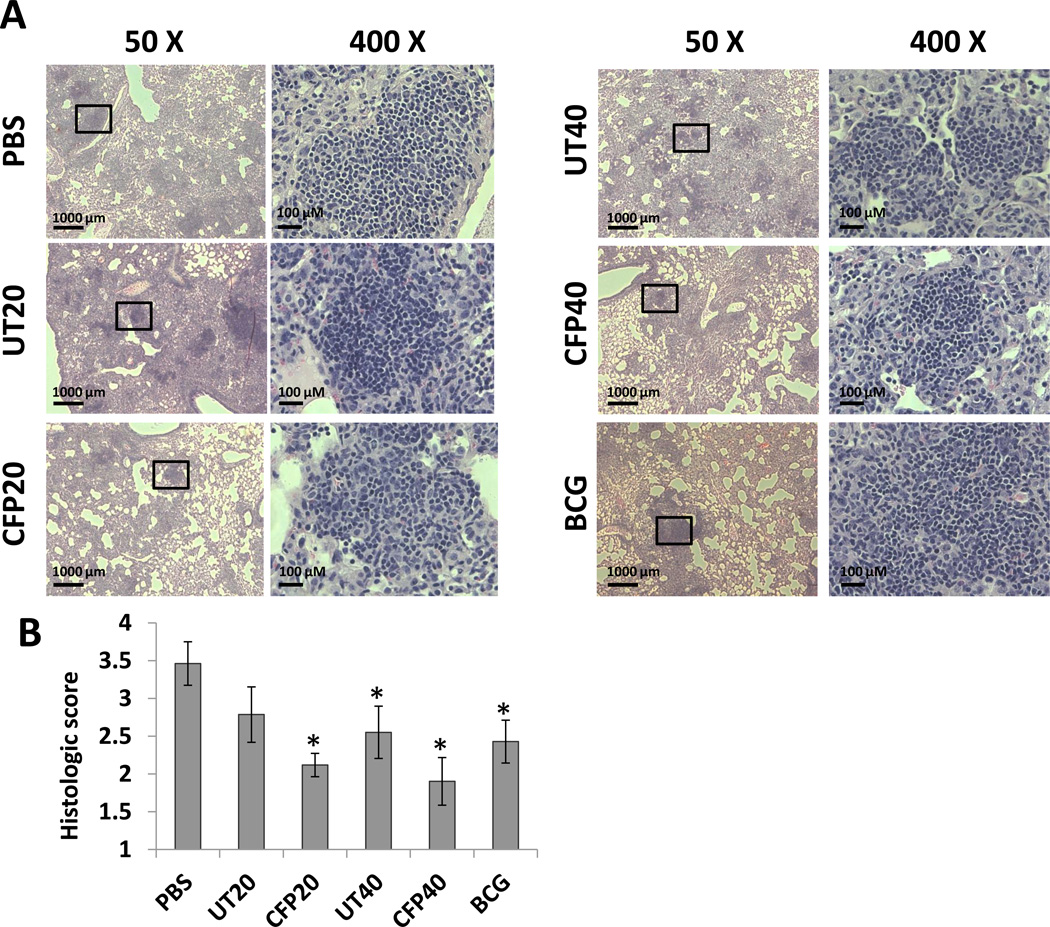
Approximately 2 billion people are infected with Mycobacterium tuberculosis, the etiological agent of tuberculosis (TB), and an estimated 1.5 million individuals die annually from TB. Presently, Mycobacterium bovis BCG remains the only licensed TB vaccine; however, previous studies suggest its protective efficacy wanes over time and fails in preventing pulmonary TB. Therefore, a safe and effective vaccine is urgently required to replace BCG or boost BCG immunizations. Our previous studies revealed that mycobacterial proteins are released via exosomes from macrophages infected with M. tuberculosis or pulsed with M. tuberculosis culture filtrate proteins (CFP). In the present study, exosomes purified from macrophages treated with M. tuberculosis CFP were found to induce antigen-specific IFN-γ and IL-2-expressing CD4(+) and CD8(+) T cells. In exosome-vaccinated mice, there was a similar TH1 immune response but a more limited TH2 response compared to BCG-vaccinated mice. Using a low-dose M. tuberculosis mouse aerosol infection model, exosomes from CFP-treated macrophages were found to both prime a protective immune response as well as boost prior BCG immunization. The protection was equal to or superior to BCG. In conclusion, our findings suggest that exosomes might serve as a novel cell-free vaccine against an M. tuberculosis infection.
Keywords: Exosomes; Mycobacterium tuberculosis; Vaccine.
© 2013 WILEY‐VCH Verlag GmbH & Co. KGaA, Weinheim.
Conflict of interest statement
Figures






References
-
- WHO. Geneva: WHO; 2012. Global Tuberculosis Report 2012.
-
- Calmette A. Sur la vaccination préventive des enfants nouveau-nés contre la tuberculose par le BCG. Ann. Inst. Pasteur. 1927;41:201–232.
-
- Kaufmann SH. Envisioning future strategies for vaccination against tuberculosis. Nat. Rev. Immunol. 2006;6:699–704. - PubMed
-
- Kaufmann SH. Future vaccination strategies against tuberculosis: thinking outside the box. Immunity. 2010;33:567–577. - PubMed
-
- Trunz BB, Fine P, Dye C. Effect of BCG vaccination on childhood tuberculous meningitis and miliary tuberculosis worldwide: a meta-analysis and assessment of cost-effectiveness. Lancet. 2006;367:1173–1180. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
